A: That is a really interesting question! What we know from the literature is that the utilization of an abdominoperineal resection with an end colostomy for rectal cancer is extremely variable when one looks at different surgeons or different centers.
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
What many of us who do a lot of rectal cancer surgery know from our practices is the same. We are sent patients with mid-rectal tumors who have been told they need a permanent end colostomy. We get sent patients with tumors that are not reconstructable who’ve been told they can have a coloanal anastomosis.
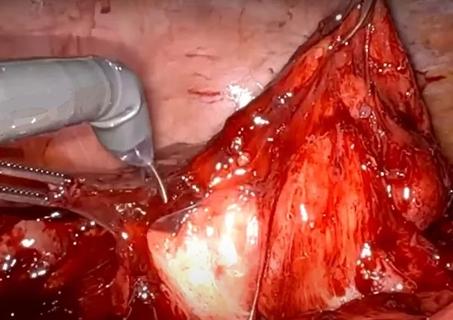
The single most important thing is that the patient has a high quality cancer operation. This means religiously following the principles of appropriate preoperative evaluation, appropriate and selective preoperative radiation or chemoradiation, and most importantly, perfect anatomical total mesorectal excision. In patients who need the anal muscle taken out, this encompasses an appropriately wide excision of the levator muscles with a cylindrical specimen, recently redescribed as an extralevator abdominoperineal resection, but actually what Sir Ernest Miles proposed and performed about 100 years ago.
In patients who can have a coloanal anastomosis, these same cancer principles are followed. But a huge amount of attention must be put into the technically perfect anastomosis ― with perfect blood supply measured by seeing pulsating bleeding from the marginal vessel ― and excellent reach of the bowel, so there is no tension on the anastomosis.
How we choose the patients who can have an anastomosis ultimately depends on patient and surgeon characteristics. If a patient is motivated to have a coloanal anastomosis, will put up with the low anterior resection syndrome and some seepage that they may have, then they are an appropriate patient. The patient needs to be able to function adequately and be mobile. They need adequate sphincters and the tumor needs to be in an appropriate location.
Having said all of that, most patients with low rectal cancer can undergo a coloanal anastomosis. For upper rectal cancers, we need a 5-cm margin with a perpendicular transection of the mesorectum. For tumors in the middle and lower thirds, this often means transecting the bowel at the ano-rectal ring. In somebody in whom I can achieve a 2-cm margin, this is the minimal margin that I will accept.
Some patients, however, will have a tumor that is below the ano-rectal ring. If I can get a 2-cm margin by coming down to the dentate line and doing an intersphincteric resection, then I will. For these patients, as long as it is not a poorly differentiated tumor and as long as we have discussed postoperative function with the patient, we can actually take a 1-cm margin and do a hand-sewn anastomosis having done an intersphincteric resection. Oncological data suggest that this is equivalent to an abdominoperineal resection in these very low tumors. Motivated patients with good sphincters can do well and enjoy the chance of avoiding a permanent ostomy.
At the end of the day, the most important thing is to make sure that your patient with a mid- or lower rectal cancer is evaluated by a multidisciplinary team who see a high volume of these patients and therefore understand the complexities of rectal cancer treatment, and individualize decision-making as is required.
Conor Delaney, MD, PhD
Chairman, Digestive Disease & Surgery Institute
Cleveland Clinic
Follow Dr. Delaney on Twitter @ConorDelaneyMD

Technique is useful in patients with diffuse stricturing Crohn’s jejunoileitis

Lifesaving procedure, continued pregnancy and healthy delivery highlight program’s advancement
Robot-assisted technique provides an alternative to open surgery in a complex case

Cleveland Clinic team blends extended mesenteric excision and Kono-S anastomosis

Continued pregnancy and delivery are only the second successful outcome worldwide

FETO and twin-twin transfusion syndrome treatments are next
New procedure eliminates volvulus risk

Measuring outcomes becomes more granular with surgeon-entered data
