Nonsurgical strategy to decompress median nerve
By Zong-Ming Li, PhD, Peter J. Evans, MD, PhD, William H. Seitz, Jr., MD, Steven Maschke, MD, David Shapiro, MD, and Yuji Umeda, MD, PhD
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In the tradition of George Phalen, MD, Cleveland Clinic’s Department of Orthopaedic Surgery and Hand Research Laboratory (Hand Lab) continue to generate insights to improve our understanding and management of carpal tunnel syndrome (CTS). We recently presented a study that offers potential breakthroughs in managing CTS at the annual meetings of the Orthopaedic Research Society and the American Academy of Orthopaedic Surgeons.
Our Hand Lab research team has been working to identify alternative strategies that relieve carpal tunnel pressure without severing the transverse carpal ligament. To this end, we have explored a novel concept that involves increasing carpal tunnel volume via the manipulation of carpal tunnel geometry and carpal tunnel mechanics.
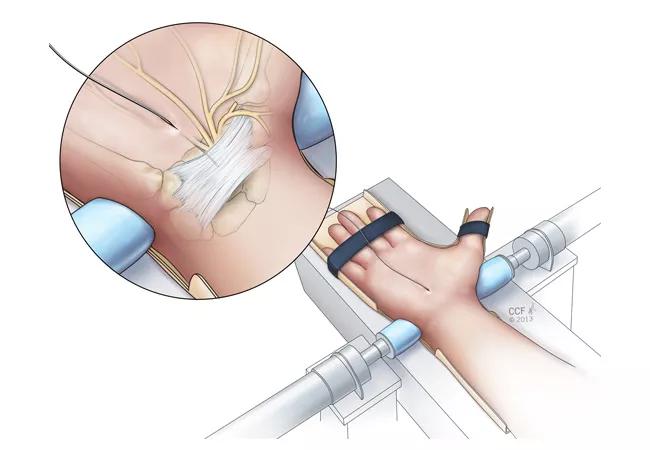
Our most recent study hypothesized that carpal tunnel pressure would decrease with the application of radioulnar wrist compression. We investigated changes in carpal tunnel pressure in CTS patients in response to carpal arch width shortened by applying radioulnar compressive force across the wrist. Six CTS patients underwent testing prior to mini-open carpal tunnel release surgery. A pressure transducer catheter was inserted into the carpal tunnel via the palmar incision to the level of the hook of hamate. With a custom compression system (Figure 1), we applied radioulnar compressive forces of 10 N and 20 N across the distal level of the carpal tunnel and recorded resulting pressure measurements. After data collection, the surgeon completed the mini-open carpal tunnel release.
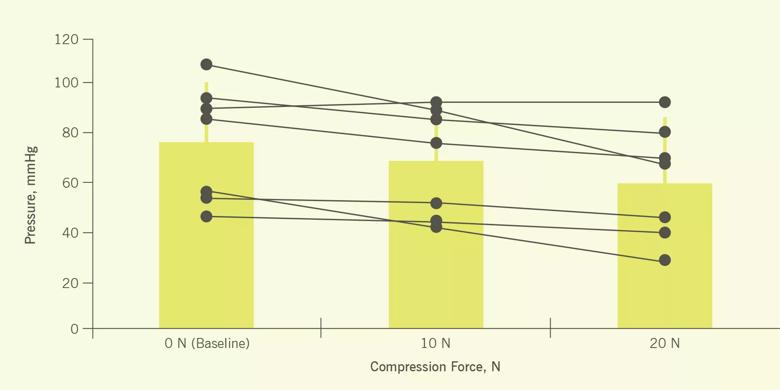
Figure 1. Schematic of carpal tunnel compression and measurement of carpal tunnel pressure
Normal pressure within the carpal tunnel is relatively low (<15 mmHg) but has been reported as high as >200 mmHg2,3 in patients with CTS. Baseline carpal tunnel pressure values of CTS patients in our study ranged from 48.2 to 106.1 mmHg.
We found that as we increased compressive force, carpal tunnel pressure decreased. (Figure 2) When the force was 10 N, carpal tunnel pressure dropped to 65.6 (SD 21.8) mmHg, a decrease of 11.0 mmHg or 14.7 percent. At 20 N, carpal tunnel pressure dropped to 59.0 (SD 23.8) mmHg, a decrease of 17.6 mmHg or 24.2 percent.
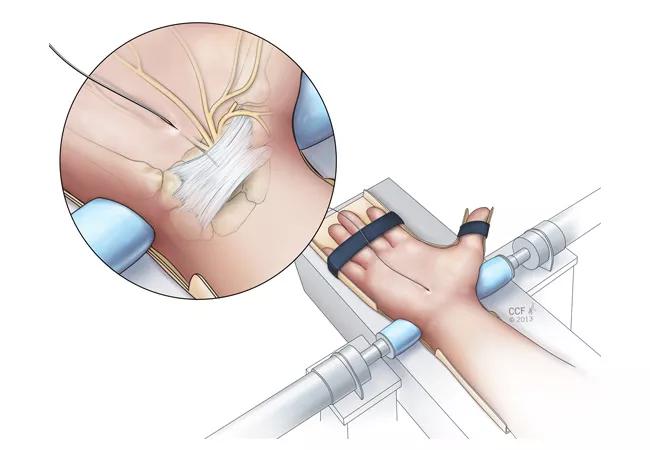
Figure 2. Carpal tunnel pressures at baseline and force applications of 10 N and 20 N for individual wrists (solid circles) and for group averages (bars).
Compressing the wrist in the radioulnar direction confirmed our hypothesis that biomechanical manipulation can reduce carpal tunnel pressure. This finding has the potential to provide an alternative, nonsurgical strategy to decompress the median nerve and improve CTS symptoms.
We are delighted that this study was awarded “Best of ORS” in the Hand and Wrist category at this year’s Orthopaedic Research Society meeting. We look forward to future research that helps define how to maximize patient-specific reduction of carpal tunnel pressure and symptom improvement by optimizing force application (e.g., magnitude, location, orientation, duration and frequency).
Other NIH-funded projects underway in our Hand Research Laboratory aim to clarify the biomechanical and neurophysiological mechanisms of sensorimotor function deficits associated with CTS. We are also identifying neural markers to detect symptoms at the earliest stages, when intervention is most effective. Our other projects have demonstrated significant changes in the thickness and stiffness of the transverse carpal ligament making up the borders of the carpal canal, which can help us better understand the etiology and diagnosis of CTS.
A half century ago, Dr. Phalen’s seminal work at Cleveland Clinic allowed us to recognize, understand, diagnose and treat CTS. Our hope is to honor his legacy through continued advances in the field.
Acknowledgements: We gratefully acknowledge the support of our carpal tunnel syndrome research program by the Orthopaedic Research and Education Foundation, Whitaker Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health.
Dr. Li is Director of the Hand Research Laboratory and Professor in the Departments of Biomedical Engineering, Orthopaedic Surgery and Physical Medicine and Rehabilitation.
Dr. Evans is Director of the Upper Extremity Center and specializes in shoulder, elbow and hand surgery.
Dr. Seitz is Professor of Orthopaedic Surgery at Cleveland Clinic Lerner College of Medicine, Chief of Orthopaedic Surgery at Cleveland Clinic Lutheran Hospital, and is President of the American Society for Surgery of the Hand.
Dr. Maschke’s special interests are hand, wrist, elbow and peripheral nerve surgeries.
Dr. Shapiro is an orthopaedic surgeon who specializes in hand surgery.
Dr. Umeda is an Associate Staff of Orthopaedic Surgery. His special interests are hand, wrist, elbow, shoulder, knee and ankle.

Cleveland Clinic specialists offer annual refresher on upper extremity fundamentals

Latest concepts in the surgical creation of functional, opposable thumbs in early childhood

CT imaging using radiopaque markers can help assess healing after surgery

Finally, a solution after multiple revision surgeries for delayed bone healing, loose hardware and unrelenting infection

Iliac crest structural autograft repairs large, uncontained defect
Two cases show multiple factors to consider

Orthopaedic oncologist discusses the complex case

Data system aims to improve orthopaedic care and drive down healthcare costs