Locations:

Cleveland Clinic team blends extended mesenteric excision and Kono-S anastomosis

Ileocolic resection is the most common surgery performed to treat intestinal Crohn’s disease (CD), yet as many as 70% of patients experience postoperative endoscopic CD recurrence.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
With recent evidence that the mesentery and its lymph nodes have important immune system functions and may exert a pathophysiologic influence in CD, two promising surgical procedures intended to reduce that potential mesenteric involvement and thus decrease CD recurrence have been developed.
Now, Cleveland Clinic researchers have shown that the two procedures can be safely and practically combined into a single surgery for primary or recurrent CD. The technique’s effect on recurrence is yet to be determined.
The new procedure is called mesenteric excision and exclusion (MEE). It blends Kono-S anastomosis and extended mesenteric excision.
Of the 22 consecutive patients who underwent MEE between September 2020 and June 2021 and were evaluated for the descriptive study, “the outcomes were very good,” says Cleveland Clinic colorectal surgeon and Inflammatory Bowel Disease Surgery Section Chief Stefan Holubar, MD, MS, the study’s first author. “Certainly they appear to be equivalent to the other types of surgeries that we do for ileocolic Crohn’s disease” in terms of minimal complications.
The mesentery is a continuous fold of membranous tissue that envelops the intestines from duodenum to rectum and attaches them to the abdominal wall. In addition to its anatomic function as a suspensive and supportive structure, and housing the blood supply and lymphatics including lymph nodes, the mesentery is increasingly recognized as a distinct organ at the interface between the intestines and the body, with the ability to mediate immunoreactivity and exert both physiologic (protective) and pathologic effects.
Advertisement
Although the etiology of CD remains unclear, there is growing evidence that the mesentery plays a role in the pathophysiology of the disease. There are mesenteric abnormalities present in CD — notably mesenteric fat wrapping and often severe thickening and hypervascularity, and the elevated expression of anti-inflammatory genes in mesenteric adipocytes. These suggest a strong linkage between endoluminal and mesenteric CD manifestation and raise the question of whether mesenteric events are precipitative rather than merely reactive in CD.
Currently, surgery is the only means of affecting mesenteric conditions. Two surgical techniques have been developed in the past decade to reduce the mesentery’s influence on luminal CD and attempt to decrease disease recurrence following ileocolic resection.
The Kono-S anastomosis (KSA) is a handsewn side-to-side anastomosis with a wide lumen that is relatively excluded from the diseased mesentery by construction of a supporting column. A randomized trial found that KSA was associated with reduced risk of postoperative recurrence of endoscopic CD compared with stapled side-to-side anastomosis.
A second surgical method called extended mesenteric excision (EME), where diseased mesentery associated with the diseased segment of ileum is resected, resulted in fewer postoperative CD recurrences in patients in a prospective case series.
The effectiveness of both procedures is still being studied in ongoing international randomized trials.
Dr. Holubar notes that KSA is the more well-established of the two techniques but is perceived as more technically demanding because it requires hand-sewing.
Advertisement
Cleveland Clinic surgeons had begun regularly performing EME with the goal of establishing a retrospective case series for future study. At the same time, Dr. Holubar was learning more about KSA and felt it could offer benefits to patients.
“A lot of people shy away from it because it’s perceived as difficult, but as someone who does a lot of hand-sewing anyway, it was very straightforward to me,” he says.
Combining the two procedures, with the goal of also combining their potential benefits, just made sense.
“I was already doing extended mesenteric excisions, and I thought, ‘OK, I’m going to do a Kono-S at the same time,’” he says. “I just naturally thought that that was what we should be offering to our patients as the most progressive, evidence-based approach.”
Combining the two procedures involves:
Figure 1. Extended mesenteric excision. ©Cleveland Clinic Foundation, 2021.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/901a8c5d-fb1a-4284-9f58-7f1dde289214/21-DDI-2438858-Mesenteric-excision-and-exclusion-01-800x550-1-150x117_jpg)
Figure 2. Supporting column construction. ©Cleveland Clinic Foundation, 2021.
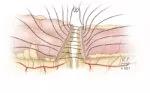
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c95e3cb2-b6c1-4045-9bc4-02c74ebccf91/21-DDI-2438858-Mesenteric-excision-and-exclusion-02-800x550-1-150x93_jpg)
Figure 3. Enterotomy construction. ©Cleveland Clinic Foundation, 2021.
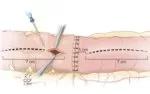
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/aca99ba5-2ab6-4fe5-9dd1-b7bdfd86679e/21-DDI-2438858-Mesenteric-excision-and-exclusion-03-800x550-1-150x94_jpg)
Figure 4. Inner layer construction. ©Cleveland Clinic Foundation, 2021.
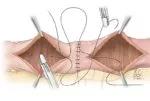
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/66603980-c00e-493e-b0e4-7a099f939d68/21-DDI-2438858-Mesenteric-excision-and-exclusion-04-800x550-1-150x101_jpg)
Figure 5. Final appearance. ©Cleveland Clinic Foundation, 2021.
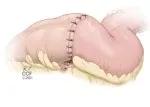
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/03336e58-d09e-4b1e-8616-e13ae4d9fd6b/21-DDI-2438858-Mesenteric-excision-and-exclusion-05-800x550-1-150x107_jpg)
The Cleveland Clinic descriptive study evaluated the 30-day outcomes of 22 patients who underwent combined MEE for either primary or recurrent ileocolic CD. Median operative time was 175 minutes. Median postoperative hospitalization was 4 days. Two of the 22 patients required readmission during the one-month postoperative period: one for a seton placement and one for percutaneous drainage of a sterile collection. There were no cases of intra-abdominal sepsis or anastomotic leaks.
Dr. Holubar and his colleagues concluded that MEE is safe and highly feasible, but further research is needed to assess whether it reduces CD recurrence.
Dr. Holubar notes that the study is a selected case series, with some patients excluded from the procedure because they were deemed inappropriate candidates for various reasons.
“If they already had one or two resections, and if the ileocolic artery was already gone, then it obviates the need” for MEE, he notes.
“You do have to pick these patients carefully, which obviously introduces an element of selection bias,” he says.
As a follow-up to the descriptive study, retrospective comparative studies of MEE and EME are underway, Dr. Holubar says. Also, “we will probably compare KSA alone and EME alone to MEE and other traditional approaches.”
Advertisement
In addition to showing the potential for better surgical options for CD, Dr. Holubar says the descriptive study’s results highlight the importance of developing and maintaining hand-sewing skills, without which he would not have been able to develop the new technique or perform other surgeries where stapling isn’t an option.
“I think it’s critically important for young colorectal surgeons to make sure that they keep hand-sewing after they graduate to fellowship and throughout their career,” he says, “because occasionally you’ll get patients where you really don’t have the luxury of being able to staple.”
Advertisement

Multidisciplinary framework ensures safe weight loss, prevents sarcopenia and enhances adherence

Study reveals key differences between antibiotics, but treatment decisions should still consider patient factors

Key points highlight the critical role of surveillance, as well as opportunities for further advancement in genetic counseling

Potentially cost-effective addition to standard GERD management in post-transplant patients

Findings could help clinicians make more informed decisions about medication recommendations

Insights from Dr. de Buck on his background, colorectal surgery and the future of IBD care

Retrospective analysis looks at data from more than 5000 patients across 40 years

Surgical intervention linked to increased lifespan and reduced complications