Locations:

Important takeaways from a rare complication
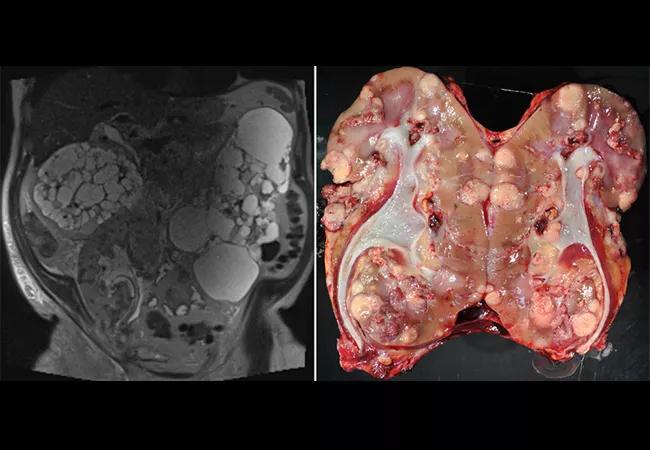
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e20e259e-58cc-48ea-84c1-1771fb9ae9ad/22-URL-2648708-CQD-650x450-1_jpg)
Donor-Derived Renal Cell Carcinoma in a Kidney Allograft: A Case
An unusual case of donor-derived renal cell carcinoma (RCC) in a kidney allograft should serve to raise awareness of the possibility, but not to discourage people from kidney donation.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
RCC in a kidney allograft is rare, with an incidence of 0.19% to 0.5%, and nearly always occurs at least a decade after transplantation. But in one patient seen at Cleveland Clinic, multifocal RCC emerged within six months of transplant and was traced to the donor kidney.
“This is a very rare complication, but such sequelae can happen. It should not discourage people from giving a kidney,” says transplant surgeon Alvin Wee, MD, of Cleveland Clinic’s Glickman Urological and Kidney Institute.
Dr. Wee and colleagues published a case report in Transplantation Proceedings. The patient was a 68-year-old man with stage V chronic kidney disease secondary to autosomal dominant polycystic kidney disease. He received a kidney transplant from a deceased donor. Graft function was excellent; and imaging, protocol biopsy and a cell-free DNA test were all normal.
Then creatinine was noted to be gradually rising at month five. Initially, Dr. Wee and colleagues suspected rejection. Donor-derived cell-free DNA had increased to 1.5% from 0.5% at month six. The transplant ultrasound showed multiple hyperechoic lesions, and further imaging with magnetic resonance imaging revealed diffuse multifocal lesions.
Percutaneous biopsy was unsuccessful; therefore, a laparoscopic-guided biopsy was done and confirmed grade 3 clear-cell RCC. Genetic testing showed that the tumor came from the donor. Allograft nephrectomy was done, and the patient was removed from all immunosuppression.
The donor was a 53-year-old male with a significant history of smoking, yet there was no hint of cancer when the organ first became available. Dr. Wee says, “When we got the kidney, we didn’t see any suspicious lesions, as most RCCs are exophytic. There was no outgrowth or bulging; and a biopsy was also done. All the parameters indicated it was a good organ as reflected from his excellent graft function after transplantation.”
Advertisement
The immunosuppression might have played a role, Dr. Wee says. “If there was a cancer cell, in theory, immunosuppression can cause these cancer cells to grow. Whether there was a cancer cell “hiding,” or was just formed, or mutated leading to the tumor, we won’t really know.”
Clinically, the case should raise awareness to include multifocal RCC in the differential diagnosis for multiple lesions in the allograft, and the use of cell-free DNA monitoring can be helpful. At Cleveland Clinic, where 306 kidney and kidney/pancreas transplants were performed in 2021, cell-free DNA is monitored routinely post-transplantation.
“When the cell-free DNA goes up, you have to be more vigilant watching the graft, as rising creatinine can be a late sign of injury. Cell-free DNA tells you there’s an injury, but not what type. That’s why additional workup may be warranted,” Dr. Wee explains.
The cancer necessitated the removal of the donor kidney, but the patient is doing well on dialysis and will soon be back on the transplant waiting list.
“We stopped the immunosuppression, and he’s fine now. Fortunately, the tumor was only in the kidney and hadn’t spread. We have to wait about two years before considering him again as a transplant candidate,” he says.
Dr. Wee adds, “We have to be vigilant. With our multidisciplinary approach, we were able to detect even the rarest occurrence and save the patient.”
Featured image: Left: Coronal T2-weighted magnetic resonance imaging series demonstrating multiple fluid-filled cysts in the native kidneys with innumerable T2 dark hypoenhancing lesions throughout the kidney allograft. Right: Gross pathology of nephrectomy specimen, renal cell carcinoma, multifocal, clear cell subtype with focal rhabdoid areas, International Society of Urological Pathology grade 4 with invasion into renal vein, renal sinus and perinephric fat, and neoplasm extending to perinephric fat margin of excision.
Advertisement
Used with permission from Elsevier. This figure originally appeared in: Gross MD, Hassanein M, Myles JL, Augustine JJ, Wee A. Donor-Derived Renal Cell Carcinoma in a Kidney Allograft: A Case Report. Transplant Proc. 2022 Jan-Feb;54(1):123-125. doi: 10.1016/j.transproceed.2021.11.017. Epub 2022 Jan 1. PMID: 34980506.
Advertisement
Advertisement

A proactive, framework-based approach

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care

Research findings offer clues for improving disease outcomes in men

Creating a safe space for patients

Long-term immune effects reshape preventative strategies and timelines

Large-scale database also reveals potential for immunotherapy to protect against cancer