Locations:

First reported imaging findings show swift reductions in perilesional edema, tumor size
Until recently, there were no targeted therapies for managing central nervous system (CNS) tumors in individuals with the autosomal dominant inherited tumor susceptibility syndrome known as von Hippel-Lindau (VHL) disease. That changed in August 2021, when the FDA approved belzutifan, a targeted inhibitor of hypoxia-inducible factor (HIF)-2α, for treatment of patients with VHL disease-associated CNS hemangioblastomas (as well as renal cell carcinomas and pancreatic neuroendocrine tumors) not requiring immediate surgery.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In the pivotal trial supporting approval of belzutifan, 63% of patients with VHL disease-associated CNS hemangioblastomas were reported to show a radiologic response, but the imaging features of this response were not shared in published trial results. To fill this gap, Cleveland Clinic clinicians recently reported imaging findings from their early experience with belzutifan — namely, two cases of VHL disease showing a strong early CNS lesion response. The findings, published as a case series in CNS Oncology, represent the first reported brain imaging studies in patients with VHL disease treated with belzutifan.
Reprinted below are pre- and post-treatment MRI findings from one of the patients, a 30-year-old white man with genetically confirmed VHL disease. He was diagnosed at age 10 after presenting with left eye vision loss secondary to retinal hemangioblastoma accompanied by brain and spinal hemangioblastomas. At age 15, he underwent surgery for a cerebellar hemangioblastoma and was monitored radiographically until age 24, when he developed posterior neck tightness, headaches and paresthesias in the extremities. Imaging showed progressive disease, which prompted resection of masses in the deep left cerebellum, the superficial cerebellum and the dorsal fourth ventricle. At age 25, imaging revealed continued disease progression in the posterior fossa, and he underwent stereotactic radiosurgery for a lesion in the left cerebellum.
Continued radiographic follow-up showed progressive disease in three cerebellar hemangioblastomas at age 29, when he was started on belzutifan 120 mg orally once daily. By his first follow-up, the patient had completed three cycles of belzutifan. Brain MRI at this time revealed interval improvement in perilesional edema and reductions in lesion diameters as follows:
Advertisement
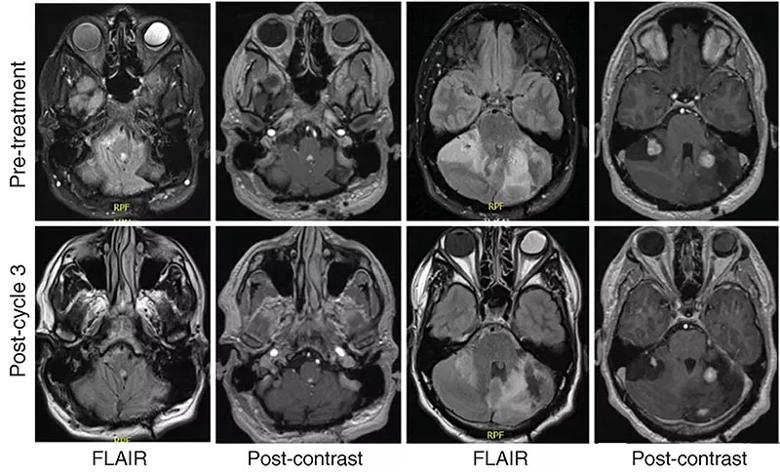
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/396c105c-2286-4f96-883f-001809285e1d/22-NEU-3216908-CQD-Inset-800x486-1_jpg)
Figure. Pretreatment (top row) and post-treatment (bottom row) MRIs of the patient, separated by an interval of four months during which he received three cycles of belzutifan. The panels show the fourth ventricular mass and several cerebellar hemangioblastomas, revealing interval reduction in perilesional edema and reduced contrast enhancement following treatment. FLAIR = fluid-attenuated inversion recovery. Reprinted from Dhawan et al., CNS Oncology (2022;11[3]:CNS91). © 2022 The Authors.
He tolerated belzutifan well, experiencing anemia with mild fatigue and dizziness but no other adverse effects. There were no new neurological deficits or findings on physical exam.
“This and the other case in our report both illustrate the swift resolution of perilesional edema associated with intracranial hemangioblastomas that can be seen after belzutifan initiation,” says the paper’s first author, Andrew Dhawan, MD, DPhil, a fellow in Cleveland Clinic’s Neurological Institute.
“While our series is limited by its small size, it illustrates the rapid initial response in CNS hemangioblastoma size and edema that can be achieved with belzutifan therapy,” adds senior author Glen Stevens, DO, PhD, a neuro-oncologist in Cleveland Clinic’s Rose Ella Burkhardt Brain Tumor and Neuro-Oncology Center. “We are pleased to contribute this initial profile of neuroradiological response to belzutifan, and we look forward to emerging evidence about response durability.”
The full case series report (open access) is available here.
Advertisement
Advertisement

For kids with painful, growing lesions in the arm, leg or pelvis

Dedicated investigators and clinicians bring expertise in drug development and flexible study design

Exploring the true prevalence of AATD among Americans and why so many remain undetected

Recommendations on identifying and managing neurodevelopmental and related challenges

National database study reveals insights into survival outcomes

Phenotypic clustering study reveals four distinct disease trajectories

Rare genetic disorder prevents bone mineralization

First-ever procedure restores patient’s health