Locations:

Avoiding abdominoperineal resection

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/fdefa716-146d-4256-a2ff-e86e9009e18f/CQD_Truong-Tufaro_Neoadjuvant-therapy_24-CNR-5148959)
Neoadjuvant therapy
A 66-year-old male presented to an outside hospital in 2019 with intermittent rectal bleeding for one year. The patient had a history of atrial fibrillation, and he had to stop his anticoagulation because of the bleeding. His colonoscopy revealed an anal mass, and the biopsy showed intestinal-type adenocarcinoma with mucinous features.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
His initial imaging including pelvic MRI showed the anal mass invading the sphincter of the anal canal. He was told he would need an abdominoperineal resection and a permanent colostomy bag.
At his first Cleveland Clinic visit, he met with Emre Gorgun, MD, staff in the Department of Colorectal Surgery at Cleveland Clinic’s Digestive Disease & Surgery Institute. “After performing a baseline flexible sigmoidoscopy, I explained to the patient that his case would be reviewed at multidisciplinary tumor board so that we could attempt to avoid abdominoperineal resection with permanent stoma bag,” says Dr. Gorgun.
During the tumor board, the surgeon, medical and radiation oncologists, and radiologist met to review pathology and imaging results and determine a course of action.
The tumor board recommended long-course neoadjuvant chemoradiation followed by restaging by with flexible sigmoidoscopy and imaging. If restaging showed a response, total neoadjuvant treatment would follow. Total neoadjuvant treatment is a novel approach for locally advanced cancer to improve the outcome of, or potentially avoid, sphincter-preserving surgery.
Dr. Gorgun discussed with the patient the multidisciplinary tumor board recommendations, and the patient was started on long course chemoradiation locally near his home.
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/450ea2fd-61c8-4a97-9075-0c2b6ddca4e8/20-DDI-2029810-Rectal-Cancer-inset_jpg)
The patient was evaluated three months later with an MRI of the rectum and flexible sigmoidoscopy in the office. There was no sign of the anal mass on the exam, and the MRI revealed a complete response to the long course of chemoradiation without residual tumor.
Advertisement
“At that time, I recommended to the patient that we proceed with total neoadjuvant treatment to see if we could reach our goal of curing the cancer without resorting to a permanent bag,” says Dr. Gorgun. The patient agreed and was scheduled for chemotherapy.
After eight cycles of chemotherapy, another MRI of the rectum showed no recurrence of the anal cancer and complete radiological response. Dr. Gorgun performed a flexible sigmoidoscopy, and it showed the scar of the treated tumor without residual tumor.
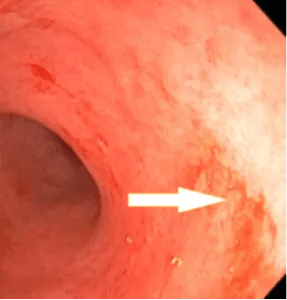
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/38d4279d-8bb8-4ee4-b84d-ff74a17efdcf/gorgun1-287x300_png)
Scar of the treated tumor without residual tumor.
His case was again discussed at multidisciplinary tumor board, and the patient was placed on a watch and wait protocol for close surveillance. With this approach, the patient will need rectal exam every three months in the office in addition to imaging and tumor markers check every six months to detect any early recurrence.
Now a year after finishing the treatment, there is no evidence of recurrence and he is compliant with his imaging. The patient preserved his rectum and sphincter and can perform his daily activities.
“This case demonstrates successful, nonoperative, organ-preserving management of a patient with locally advanced cancer,” says Dr. Gorgun. “Our multidisciplinary approach was key to this outcome, with each specialist playing an important role in determining the best course of action for this patient. This is the approach we take to all patients at Cleveland Clinic as we believe it gives our patients the best chance at a positive outcome.”
Advertisement
Advertisement

A proactive, framework-based approach

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care

Research findings offer clues for improving disease outcomes in men

Creating a safe space for patients

Long-term immune effects reshape preventative strategies and timelines

Large-scale database also reveals potential for immunotherapy to protect against cancer