Locations:

Improving outcomes and simultaneously decreasing costs

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/5ab054b8-bd19-4d25-82cb-e509b0211a59/17-ORT-1245-Billow-Hero-Image-650x450pxl_jpg)
17-ORT-1245-Billow-Hero-Image-650x450pxl
By Damien G. Billow, MD; Cesar M. Cereijo, DO; Daniel Worrell, DO; Michael Okrent, ScD; and Christopher Whinney, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Hip fractures are a common orthopaedic problem that is becoming more prevalent as our country’s population continues to age. Hip fractures most commonly occur in elderly patients and have a known morbidity and mortality associated with them. In addition to the significant effect they have on the patient, they also come at a significant price to both hospital systems and society. Complications, mortality and costs are known to be less when surgery is performed in less than 48 hours.
Using a multidisciplinary team approach, we developed a protocol for the preoperative evaluation and optimization of elderly hip fracture patients to increase the percentage of getting patients to the operating room in less than 48 hours. By doing so, we improved outcomes and decreased hospital costs.Patients 65 years or older with a hip fracture were enrolled in our protocol. Patients with prior surgery to the affected hip, pathologic fractures and those who refused surgery were excluded. All patients received a standard laboratory and radiographic workup. Chest X-rays, deep vein thrombosis duplex ultrasounds, internal medicine and anesthesia consults were obtained based on agreed-upon indications. Other consultants, such as cardiology and pulmonary, were obtained at the discretion of internal medicine staff. Time frames were established for evaluation by consultant services (Table 1). A customized history and physical note and order set were created and embedded in our electronic medical record (EMR).
Advertisement
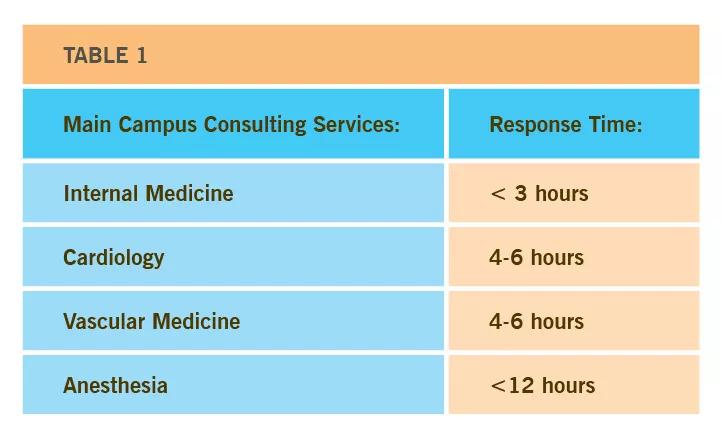
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/dcef97d6-4ba1-47c9-8fbd-9487608860a1/17-ORT-1246-Billow-Inset-Table-01-650pxl-width_10_09_2017_jpg)
Patients were enrolled into our protocol from August 2016 through March 2017 and compared to a similar population from the preceding 10 months. Outcome measures were collected from our institutions EMR and included time to surgery, hospital length of stay, patients to surgery <48 hours, in-hospital mortality, 30-day mortality and readmission, 90-day mortality and readmission, intensive care unit (ICU) admission and length of stay, in hospital complications, and consult times. Our institute’s finance director obtained information on total direct cost to the hospital.
Twenty-six patients were consecutively enrolled in our pilot cohort and compared to 43 patients in the pre-pilot cohort. The two groups were similar in regards to Charlson Comorbidity Index, age, ASA class and treatment by 13 various surgeons (Table 2).
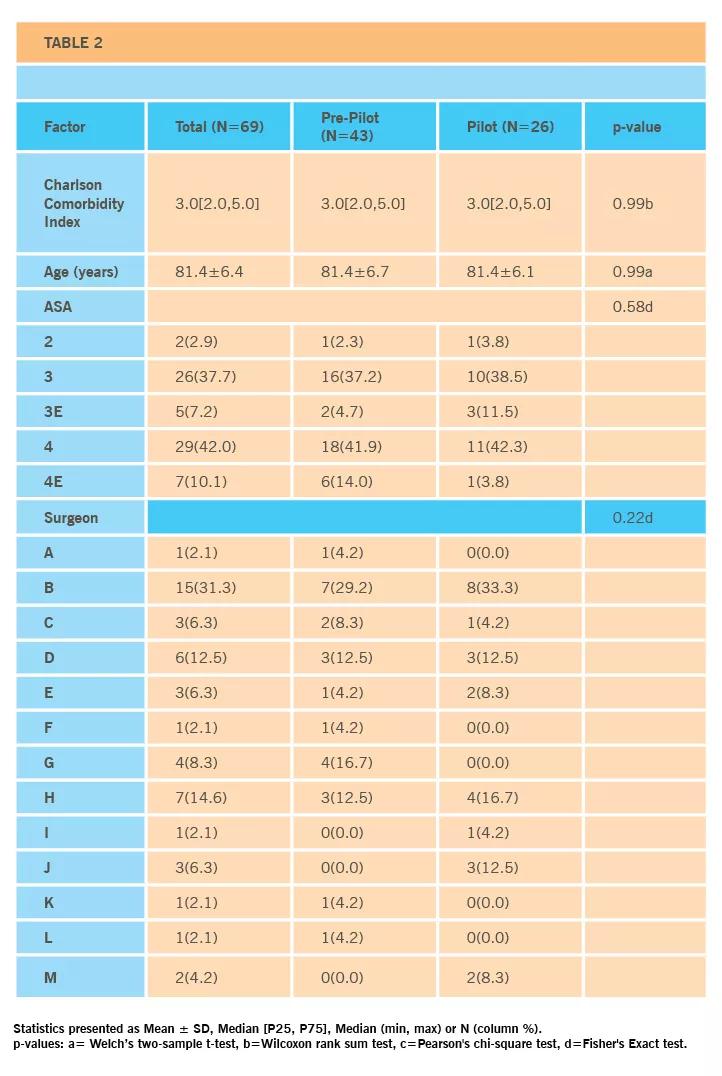
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/eb6b3f36-d35f-43f7-a092-3a4b5b1b9544/17-ORT-1246-Billow-Inset-Table-02-650pxl-width_10_09_2017_jpg)
For those patients requiring an internal medicine consult, there was a significant decrease in time to evaluation in the pilot group. Consult time was shortened from 8.8 hours to 3.5 hours (p<0.001). Cardiology consult time was also decreased by 8.4 hours in patients requiring cardiology evaluation of preoperative optimization (p=0.011).
Secondary to this, median hours to surgery decreased from 34.0 to 23.0 (p=0.077) and percent of patients who went to surgery in less than 48 hours increased from 67.4 percent to 88.5 percent (p=0.082).
Length of stay decreased by 1.2 days after implementation of the protocol from a median of 7.6 days in the pre-pilot cohort to a median of 6.4 days in the pilot cohort (p<0.23).
Advertisement
Of the 43 pre-pilot patients, 16 (37.2 percent) required postsurgical ICU admission. Pilot cohort postsurgery ICU admission rates were significantly lower with admission of only 11 percent of patients to the ICU (p<0.05).
In-hospital mortality also decreased from 9.3 percent in the prepilot cohort to 0 percent in pilot group (p=0.29). At 30 days, mortality decreased by 7.8 percent in the pilot group (p=0.40) from 11.6 percent to 3.8 percent. Ninety-day mortality rates were significantly lower in the pilot cohort compared to the pre-pilot cohort (3.9 percent and 27.9 percent respectively, p<0.05).
Hospital readmission was also assessed at 30 and 90 days postoperatively and was down in all groups.
Postoperative complications, including pressure ulcers, pneumonia, pulmonary emboli and deep vein thrombi, were taken into account. Although there was a decrease among all, there was no significant difference in either group.
There was a 26.1 percent decrease in average direct cost to the hospital per hip fracture patient after implementation of the protocol between the pre-pilot and pilot groups.
In summary, by developing and implementing a multidisciplinary protocol for preoperative evaluation and optimization of elderly hip fracture patients, we were able to get patients seen earlier by consultant services and operated on sooner. This led to decreased ICU admissions, decreased length of stay, decreased in hospital, 30-day and 90-day mortality rates, decreased 30-day and 90-day readmission rates and at a 26.1 percent decrease in average direct cost to the hospital. This was made possible by great team work and cooperation from physicians across multiple disciplines.
Advertisement
Dr. Worrell is a resident; Dr. Okrent, is in the Continuous Improvement Department, and Dr. Cereijo is a fellow at Vanderbilt University School of Medicine.
Featured image: AP image of a sliding hip screw device in a 91-year-old female.
Advertisement
Advertisement

New research highlights serious risks and the critical need for earlier advance care planning

Initiatives focus on the physical and emotional well-being of geriatric patients and their caregivers

Researchers explore the mental and physical benefits of social prescribing

Multidisciplinary approach helps address clinical and psychosocial challenges in geriatric care

Effective screening, advanced treatments can help preserve quality of life

Study suggests inconsistencies in the emergency department evaluation of geriatric patients

Auditory hallucinations lead to unusual diagnosis

How providers can help prevent and address this under-reported form of abuse