Locations:

Team prevents amputation and leaves femoral head intact

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/08f37c13-0533-4391-b1aa-51d96e73a9ea/21-ORI-2349797-CQD-650x450-1_jpg)
21-ORI-2349797 CQD 650×450
Neoadjuvant chemotherapy and an expandable prosthesis helped Cleveland Clinic’s multidisciplinary sarcoma team preserve the leg of a young girl and maintain her function following resection of a very large femoral osteosarcoma.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“It was a challenging reconstructive case,” says orthopaedic surgeon Lukas Nystrom, MD. “The novel aspect is how much of her femur we removed. We were still able to use the implant without doing a total femur replacement.”
When the patient presented in early 2020, she had pain and swelling and could not fully bend her knee. She was diagnosed with an osteosarcoma measuring 26 cm long. (Any dimension greater than 8 cm is considered “large” by American Joint Committee on Cancer criteria.)
The team initially thought amputation would be necessary. Chemotherapy was started while the parents deliberated.
“Usually we give chemotherapy, then take a break to perform surgery, and then give more chemotherapy,” explains Dr. Nystrom. “But this patient got a full chemotherapy regimen before surgery, while her parents were considering amputation. After the course of chemotherapy, the tumor had shrunk and solidified to the point where we thought it was reasonable to try to save the patient’s leg. So, we actually changed our recommendation.”
In December 2020, Dr. Nystrom and Nathan Mesko, MD, Center Director, Orthopaedic Oncology, and Director of Sarcoma Care at Cleveland Clinic, collaborated to remove the tumor, carefully preserving the patient’s femoral head and neck. They implanted a JTS® Extendible Distal Femoral Implant (Stanmore), hoping that the femoral head would continue to grow and allow the acetabulum to develop. If the femoral head had been removed, the acetabulum would cease developing.
Advertisement
“Retaining the femoral head was preferable,” says Dr. Nystrom. “A total femur replacement would require detaching surrounding tendons and reattaching them to metal, which really impacts the ultimate function of the hip.”
The surgical team waited six months for the implant site to heal. Since then, the prosthesis has been expanded twice (Figures 1 and 2).
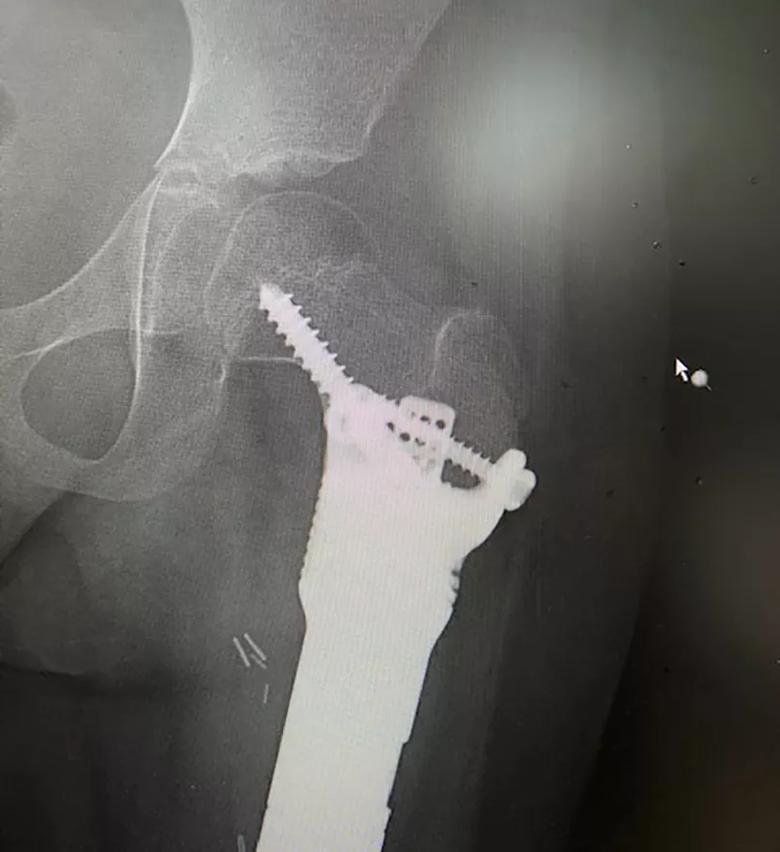
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6689842d-e3cd-4ed7-85ad-fc4f782cf665/21-ORI-2349797-Inset1_jpg)
Figure 1. AP radiograph of the hip at three months post-surgery, showing fixation of the massive expandable endoprosthesis to the short segment of proximal femoral bone. Fixation is aided by hydroxyapatite-coated surfaces, antirotational fins and screws.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c1cdc4f7-bc7e-4804-baf7-c253d469450a/21-ORI-2349797-Inset2-768x1024_jpg)
Figure 2. AP radiograph of the proximal femur showing the fixation remaining strong eight months after surgery. The gap that can be seen along the prosthesis represents the 5 mm of expansion that occurred after the first lengthening procedure.
The child’s knee is placed in a magnetic ring. The magnet spins a device inside the implant, which turns a screw and lengthens the device in a controlled fashion. The procedure is done noninvasively in an exam room, without anesthesia. The patient feels only slight stiffness due to the stretching.
This lengthening procedure will be repeated every two to three months until the patient is fully grown, around age 14.
“We’ll monitor the growth of her other leg and try to match it,” says Dr. Nystrom. “Once that growth plate closes, we’ll stop. If we estimate incorrectly and overlengthen the prosthesis, we also can reverse the process and shorten the leg.”
Advertisement
Today the patient is doing well, able to walk, ride a bike, go to school and play actively.
“We advise kids with these prostheses not to do high-impact activities, like running or sports that involve a lot of jumping,” says Dr. Nystrom. “Swimming, cycling, walking and other low-impact activities are totally fine.”
Dr. Nystrom credits Cleveland Clinic’s multidisciplinary sarcoma team, including pediatric oncologists and child life specialists, for this patient’s positive outcome.
“It has been a true team effort,” he concludes.
Advertisement
Advertisement

A proactive, framework-based approach

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care

Research findings offer clues for improving disease outcomes in men

Creating a safe space for patients

Long-term immune effects reshape preventative strategies and timelines

Large-scale database also reveals potential for immunotherapy to protect against cancer