Locations:

The clinical picture
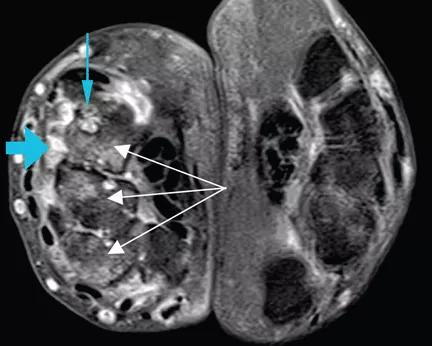
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/abd09203-c181-442d-83d7-7d1bbe7e754f/RTEmagicC_Kochhar_WhippleDisease_F1_gif_gif)
RTEmagicC_Kochhar_WhippleDisease_F1.gif
By Gursimran S. Kochhar, MD, Maged Rizk, MD, Deepa T. Patil, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 47-year-old man who had been diagnosed with rheumatoid arthritis 5 years previously was referred to us for management of bilateral pleural effusions. At the time of his diagnosis, his symptoms included pain and swelling of both wrists and the metacarpal joints of both hands. His serum C-reactive protein level had been elevated at that time, but he had no detectable rheumatoid factor. Findings on magnetic resonance imaging of the hand were very suggestive of rheumatoid arthritis (See image above: Axial T1-weighted magnetic resonance imaging with gadolinium contrast shows synovitis (large blue arrow) along the dorsal aspect of the wrist. Also seen are erosions in the carpal bones (thin blue arrow) and bone marrow edema (white arrows), which is asymmetrical compared with the other wrist, a finding highly suggestive of rheumatoid arthritis.). He had been started on the anti-tumor necrosis factor agent etanercept but his symptoms improved only slightly, and therefore a glucocorticoid had been added. Two years later, he developed abdominal pain, for which he underwent cholecystectomy. However, he continued to have chronic, generalized abdominal pain, and over the next 4 years he lost 25 lb. Upper endoscopy showed no mucosal changes, and multiple random biopsy samples were obtained for histologic evaluation (Figure) as part of his workup for chronic abdominal pain.
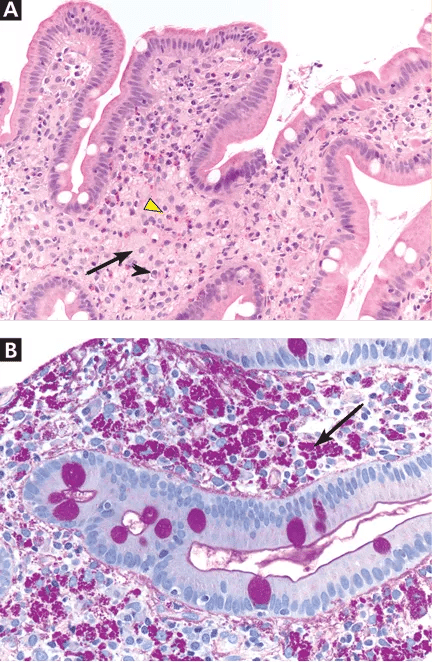
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2e184f1e-14bb-4ae7-80e0-36cde2879aca/RTEmagicC_Kochhar_WhippleDisease_F2_gif_gif)
Figure. (A) The duodenal mucosa shows expansion of the lamina propria by “foamy“ macrophages (black arrow) admixed with eosinophils (yellow arrowhead) and plasma cells (black arrowhead) (hematoxylin and eosin, × 100). (B) Periodic acid-Schiff staining with diastase digestion reveals foamy macrophages containing diastase-resistant bacilli (arrow) (× 200).
Advertisement
A: As shown in the figure above, staining of duodenal specimens showed intact villous architecture, with focal expansion of the lamina propria by “foamy” macrophages, rare plasma cells, and eosinophils, a key feature of Whipple disease. Periodic acid-Schiff staining showed numerous bacilli within the macrophages, thus confirming the diagnosis of Whipple disease. The diagnosis was also confirmed by polymerase chain reaction testing. Staining for acid-fast bacilli was negative.
Whipple disease is a rare systemic disease with a very low incidence rate worldwide. Thus, its prevalence is difficult to estimate accurately. It is caused by a gram-positive bacterium, Tropheryma whippelii.1,2 The typical clinical manifestations are diarrhea, abdominal pain, weight loss, and fever. In most patients, these are often preceded by articular symptoms,3 as in our patient, who had articular symptoms for 5 years before he was diagnosed with Whipple disease.
Interestingly, our patient also had pleural effusion, which is uncommon in Whipple disease.4
The pathogenesis of Whipple disease is thought to be related to bacterial replication within macrophages, which leads to a systemic immune response and tissue infiltration by the organism.5 Histologic evaluation is the most common way to confirm the diagnosis.
As our patient’s disease course illustrates, Whipple disease should be part of the differential diagnosis of arthritis, as antibiotic therapy alone leads to a dramatic clinical response.
Our patient was started on a 2-week course of intravenous ceftriaxone followed by oral sulfamethoxazole and trimethoprim, and his abdominal and articular symptoms completely resolved within 4 weeks.
Advertisement
This article originally appeared in the Cleveland Clinic Journal of Medicine, 2013 May;80(5):272-273.
References
Advertisement
Advertisement

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support

Research demonstrates cirrhosis regression in one-third of patients, with higher rates using alternative assessment