Locations:

Components separation returns viscera to abdominal cavity
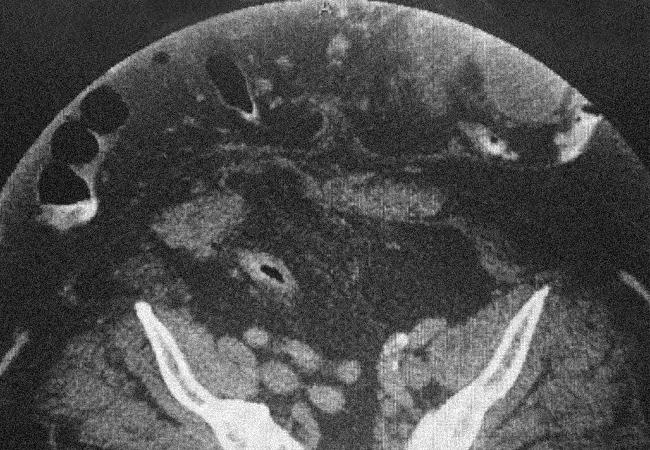
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cd0ff2f2-e614-44bb-847f-5a412809e113/17-DDI-3986-Hernia-Vignette-CQD-Hero_jpg)
17-DDI-3986-Hernia-Vignette-CQD-Hero
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Loss of domain is defined as a clinical situation when more of the viscera is outside the abdominal cavity than inside.1 This can make closure of the fascia impossible, or can result in elevated intra-abdominal pressures leading to abdominal compartment syndrome.
The operative management of these patients can be quite challenging and is debated in terms of technique. Components separation, or release of the abdominal wall musculature, is one approach that can provide additional space to return the viscera to the abdominal cavity.
The patient is a 61-year-old male with a BMI of 50, multiple prior venous thrombotic events, and history of two prior ventral hernia repairs. He developed a recurrence of his hernia with significant loss of abdominal domain. He then developed small bowel obstruction which was refractory to nasogastric decompression.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1006c194-35d8-4fef-8423-546080b8dc47/17-DDI-3986-Hernia-Vignette-CQD-Inset3_jpg)
Saggital view of CT scan demonstrates more visceral content outside of the abdominal cavity than inside the abdominal cavity.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/45b8f547-5fda-4bd4-88f7-9fc19e670067/17-DDI-3986-Hernia-Vignette-CQD-Inset2_jpg)
Preoperative preparation: This picture demonstrates loss of domain with compromised skin and soft tissue on top of the hernia defect.
Due to loss of domain, the patient’s body habitus, and expected complexity of his operation, he was not considered to be a candidate for surgery locally. He was discharged to home, obstructed, on TPN from his local hospital.
He travelled from Texas to Cleveland Clinic for further evaluation while starting to recover from his obstruction. Only tolerating liquids by mouth, he was evaluated in the office and booked for surgery the following week. His obstruction was relieved and his abdominal wall was fully reconstructed with a component-separation technique2, using four pieces of synthetic mesh sewn together measuring 52 cm x 62 cm, to reinforce the repair.
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f9edbb60-78ff-41f7-8e7d-d67806dfc207/17-DDI-3986-Hernia-Vignette-CQD-Inset4_jpg)
Four large pieces of synthetic mesh were sewn together in order to fully reconstruct the abdominal wall and reinforce the repair.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/42e673d6-8f30-4a91-96d3-5e3af60c174a/17-DDI-3986-Hernia-Vignette-CQD-Inset5_jpg)
Postoperative view: Once the abdominal wall was reconstructed, a substantial amount of redundant skin and soft tissue was resected to mitigate risk of wound ischemia and secondarily to improve cosmesis.
His postoperative course was uneventful, and he was able to go home two weeks after discharge from the hospital. He had a minor wound issue at home, which we were able to evaluate and treat through a “virtual” visit. The patient continues to recover well at home.
References
Advertisement
Advertisement

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support

Research demonstrates cirrhosis regression in one-third of patients, with higher rates using alternative assessment