Locations:

Anticoagulants don’t decrease survival or raise LGB risk

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/b3e52c4a-cca0-43da-94fa-0156df29018a/17-DDI-499-GI-Bleeds-CQD_jpg)
17-DDI-499-GI-Bleeds-CQD
In the past decade, the number of renal transplants performed has risen, resulting in both increasing life expectancy and complications in these patients.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Yet there remained a dearth of good data and evidence-based guidance on the management of renal transplants recipients, especially with regard to lower gastrointestinal bleeding. A group of six Cleveland Clinic researchers recently undertook the largest study to date addressing these gaps, which was published in Transplantation Proceedings.
Gokhan Ozuner, MD, a colorectal surgeon at Cleveland Clinic’s Digestive Disease & Surgery Institute and the primary author of the study, says, “The main findings were (A) that a nonfunctioning kidney was a negative. Transplant recipients with a nonfunctioning kidney were more likely to experience a lower GI bleed (LGB) and have a poor overall outcome; and (B) that taking an anticoagulant did not decrease overall survival or increase the risk of lower GI bleed.”
Dr. Ozuner explains that the second finding debunks a long-standing assumption among many clinicians that patients taking anticoagulants or immune-suppressants would have worse outcomes after a renal transplant. “It’s a dogma or a myth that people believe in,” he says. “But we did not find out that this is true. We were surprised.” In this study, transplant recipients who took anticoagulants did not have lower overall survival rates or an increased risk of lower GI bleed than recipients who were not taking anticoagulants.
The researchers worked with a sample of 1,578 renal transplant recipients with a mean age of 50 plus-or-minus 14 years at the time of transplantation, of which 62.5 percent were male. The mean follow-up time to assess outcomes and complications after transplantation was 57 plus-or-minus 45 months. Forty-five, or 3 percent, of the patients were diagnosed with lower gastrointestinal bleeding, and the mean time to the onset of such bleeding was 43 plus-or-minus 36 months.
Advertisement
Those patients who were taking anti-aggregant or anti-coagulant medications were at no heightened risk for lower gastrointestinal bleeding; however, a nonfunctioning graft was associated with such lower GI bleeding. Furthermore, renal transplant recipients who did experience lower GI bleeding had a higher overall mortality rate, not directly related to the bleeding episode, in comparison with transplant recipients who did not experience lower GI bleeding.
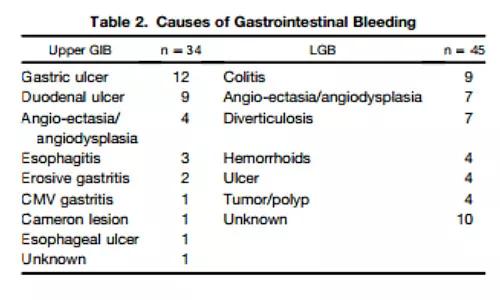
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/86685c36-1a6c-4fdb-80c5-393cd8cc6fc4/17-DDI-499-GI-Bleeds-CQD-Inset_jpg)
The study’s authors conclude that, because a patient’s having a nonfunctioning graft proved to be a risk factor for lower GI bleeding and is also associated with poor overall survival, the use of strategies to prolong the function of transplanted kidneys may lower the incidence of lower GI bleeding and extend life expectancy for patients with transplanted kidneys.
Advertisement
Advertisement

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support

Research demonstrates cirrhosis regression in one-third of patients, with higher rates using alternative assessment