Locations:

Changes lowered IBP rate by 10 percent

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3101aac9-080c-4f3e-afba-3c67222028d7/CCC_5960858_03-06-25_1834_AMO)
Colonoscopy
Every year in the United States, 12 million patients undergo colonoscopy, many for colorectal cancer screening or polyp surveillance with an aggregate cost of $19 billion.1 More than 25 percent of patients undergoing colonoscopy are reported to have inadequate bowel preparation (IBP).2 This reduces the odds that precancerous colorectal lesions will be found on exam and typically requires repeat colonoscopy at a shortened interval.3 Previous studies have demonstrated that having IBP on the first colonoscopy increases the risk of having IBP on the second exam.4, 5
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
With this in mind, researchers recently undertook a study to determine factors associated with IBP on the second colonoscopy in patients with IBP on baseline colonoscopy. “These patients are high-risk to begin with so you want to do everything you can to reduce the risk of IBP to make sure they have a successful second colonoscopy,” says Shashank Sarvepalli, MD, Internal Medicine, Cleveland Clinic.
Dr. Sarvepalli is first author on the study and presented the results today on behalf of colleagues in the Departments of Gastroenterology, Internal Medicine and General Surgery at the 2018 American College of Gastroenterology annual meeting.
The investigators looked at the records of 4,677 Cleveland Clinic patients who required repeat colonoscopy due to IBP on their first colonoscopy. They found that 32 percent had IBP on their second exam. Fifty percent of the patients were male and the mean age was 60.
After controlling for confounding factors, Dr. Sarvepalli and colleagues discovered three modifiable factors that were inversely associated with IBP on the second colonoscopy: use of a low volume (< 4L) rather than a high-volume (4L) commercial bowel preparation, having the second colonoscopy the day following the first colonoscopy, and having the procedure before noon.
Some providers prescribe high volume bowel preparations to their high-risk patients to achieve better cleansing for the second colonoscopy. However, this study demonstrated that giving these patients a low volume bowel preparation was associated with reduced IBP. “It is possible that patients — especially in the ambulatory settings — may be more likely to tolerate and complete a lower volume preparation which may reduce the odds of IBP,” Dr. Sarvepalli says.
Advertisement
Using a statistical tool called counter-factual analysis, they were able to show that with all three of these changes (using low volume bowel preparation, scheduling the second colonoscopy the day after the baseline exam with IBP and before noon), the rates of IBP rate would be 10 percent lower.
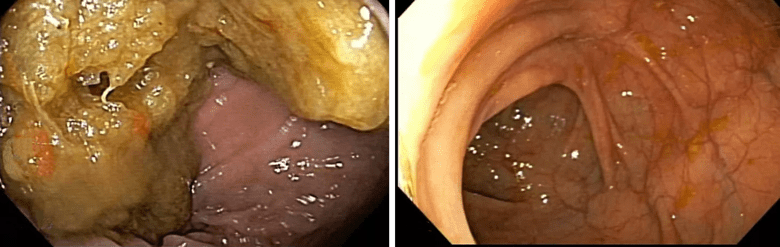
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/53333af1-fba2-451a-87b1-8cd036412225/colon_png)
Image left depicts a dirty colon while image right depicts a clean colon.
Dr. Sarvepalli and his colleagues say their model showed that if all three modifications had been undertaken in the cohort, the IBP rate would have dropped from 32 percent to 22 percent.
“That’s a substantial drop,” he says. “Our message to providers is that when you’re ordering a repeat colonoscopy, if you just follow these three simple measures, you may be able to make a substantial dent in the number of people who go on to have a second inadequate bowel preparation.”
1. Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143(5):1179-87.e1-3.
2. Woo DH, Kim KO, Jeong DE, Nam YJ, Lee SH, Jang BI, et al. Prospective analysis of factors associated with inadequate bowel preparation for colonoscopy in actual clinical practice. Intest Res. 2018;16(2):293-8.
3. Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75(6):1197-203.
4. Rex DK. Optimal bowel preparation — a practical guide for clinicians. Nature Reviews Gastroenterology & Hepatology. 2014;11(7):419-25.
Advertisement
5. Ben-Horin S, Bar-Meir S, Avidan B. The outcome of a second preparation for colonoscopy after preparation failure in the first procedure. Gastrointest Endosc. 2009;69(3 Pt 2):626-30.
Advertisement
Advertisement

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support

Research demonstrates cirrhosis regression in one-third of patients, with higher rates using alternative assessment