Locations:

TaTME's uses now extends beyond rectal cancer
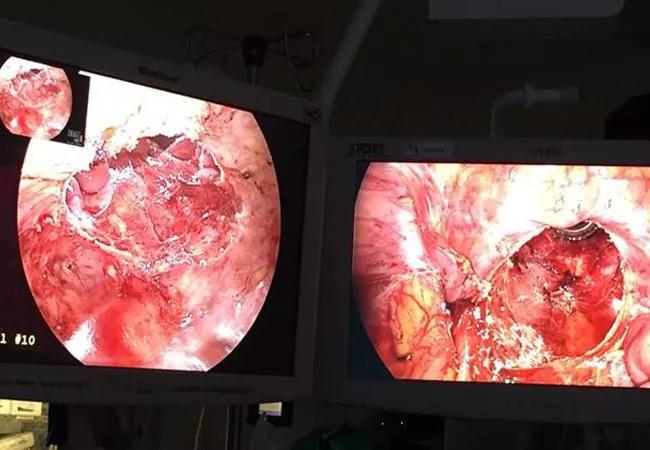
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c33ea7c1-1a7f-4af8-b1ff-c0e63fc5e7b8/18-DDI-5838_2_CQD_650x450_jpg)
18-DDI-5838_2_CQD_650x450
Taking something challenging and making it easier sometimes requires a different approach. This now holds true for surgery to remove rectal cancer in many patients.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Historically, surgeons take a ‘top down’ strategy — entering the abdomen first and then dissecting and working their way downward toward the pelvis. This technique, however, carries some inherent challenges, including ones so great that surgeons sometimes have to stop before surgery is complete.
Taking a different angle — literally — is Cleveland Clinic Florida colorectal surgeon Dana Sands, MD.
Transanal mesorectal total excision (TaTME) of rectal cancer is an approach where she starts from the bottom — through the anus — and dissects up through the pelvis.
“We’re taking the hardest part of the dissection, the lower part, and put it right at our fingertips,” she says.
Not only is Cleveland Clinic a leading center for TaTME in the United States, Dr. Sands has one of the highest single surgeon experiences using TaTME for rectal cancer. She has proctored surgeons from around the world in the technique.
TaTME for rectal cancer has been so successful, in fact, that Dr. Sands expanded the technique to many other complex pelvic surgery patients.
Armed with the experience from nearly 100 TaTME procedures for cancer, Dr. Sands is treating people with chronic pelvic infections, colostomies that need to be closed and others with a history of failed pelvic reconstruction.
“We’ve taken this TaTME approach and made some of the most difficult surgical cases that colorectal surgeons face exponentially easier,” she says. “I get patients now who are referred for surgery who have been turned down by other surgeons. In some cases, the surgeon backed out of the surgery because they couldn’t get to the pelvis from above, through the abdomen.”
Advertisement
In addition to the greater ease associated with a ‘bottom up’ or transanal approach, smaller incisions and shorter length of stay for patients are potential advantages compared to traditional abdominal approaches to pelvic surgery, she says.
Dr. Sands and colleagues expected a recent complex case to take all day and booked the operating room accordingly, for example. “But by 11:30 in the morning, we were done and thought ‘Wow, that was so easy compared to what it should have been.’”
Total mesorectal excision (TME) has remained the standard of care for treatment of rectal cancer years for many decades. Over time, the approach evolved from a big open incision across the abdomen to laparoscopic and even robotic procedures.
One constant was surgeons starting at the abdomen and working their way down into the pelvis.
“The concept of TME is really important in rectal cancer surgery, and we have known this for a long time,” Dr. Sands says. “The problem and the challenge are accessing the pelvis in people who have a narrow pelvis to begin with — the dissection can be really challenging.”
For patients with a history of major abdominal procedures, the traditional approach through scar tissue and adhesions presents additional challenges. Using TaTME, surgeons can avoid such a ‘hostile abdomen’ altogether in some cases. “Our approach turns this completely around and oftentimes we don’t even have to enter the abdomen.”
“It’s been a great experience for me,” Dr. Sands says. “It’s a perfect approach for these complicated surgeries and situations that most people cannot fix.
Advertisement
Dr. Sands recommends physicians refer their challenging rectal cancer and pelvic surgery patients to a center with experience performing TaTME. At Cleveland Clinic’s main campus, TaTME is also performed by Conor Delaney, MD, PhD; Scott Steele, MD; I. Emre Gorgun, MD; Matthew Kalady, MD; and Bradley Champagne, MD.
Data is forthcoming on the importance of routinely performing such procedures. “We’re getting ready to publish our learning curve experience on our first 85 patients.”
TME and TaTME specifically are likely to continue evolving, she says. “As new technology comes out, like a transanal robotic platform that is coming out, there will be ways to expand even upon the technology we have now.”
Advertisement
Advertisement

Findings may help guide earlier AUD intervention

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support