Locations:

The when and how of surgical interventions, and how symptoms may predict likely outcomes
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Podcast content: This podcast is available to listen to online.
Listen to podcast online (https://www.buzzsprout.com/2243576/13584759)
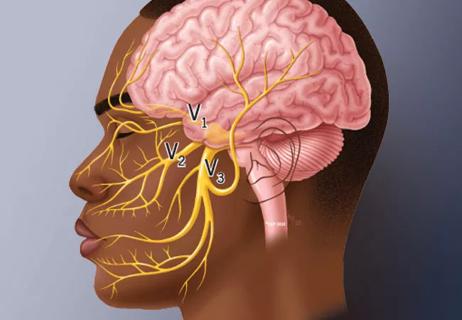
As a neurosurgeon specializing in skull base and cerebrovascular disorders, Varun Kshettry, MD, sees plenty of dramatic clinical presentations. Even so, one of his other specialty interests — trigeminal neuralgia — remains particularly striking to him. “An episode is like getting electrocuted in the face,” he says. “So being able to investigate and help some of these patients get out of that state of pain can be very rewarding and fascinating.”
Dr. Kshettry brings that experience to bear as surgical director of Cleveland Clinic’s trigeminal neuralgia program. In the latest episode of Cleveland Clinic’s Neuro Pathways podcast, he discusses surgical interventions for trigeminal neuralgia, covering the following:
Click the podcast player above to listen to the 31-minute episode now, or read on for a short edited excerpt. Check out more Neuro Pathways episodes at clevelandclinic.org/neuropodcast or wherever you get your podcasts.
This activity has been approved for AMA PRA Category 1 Credit™ and ANCC contact hours. After listening to the podcast, you can claim your credit here.
Dr. Kshettry: I always try to educate patients that there is a spectrum of facial pain and a spectrum of trigeminal neuralgia. And for any given patient, I try to figure out where on this spectrum their pain appears to be. Now, trigeminal neuralgia is a clinical diagnosis, so I tell them there are no imaging or blood tests that will actually verify that their pain is trigeminal neuralgia. The diagnosis depends on the symptoms.
Advertisement
To simplify it from a proceduralist standpoint, we have a spectrum where on one side we have classic trigeminal neuralgia symptoms. Those patients tend to have the highest success rates with our procedures. In the middle of the spectrum we have trigeminal neuralgia with atypical features, where the majority of the symptoms are classic but there are a couple features that are atypical. Those patients tend to have lower chances of success but still decent results. Then, on the other side of the spectrum, we have atypical facial pain ― or the term “idiopathic persistent facial pain” ― and a whole host of other types of face pain that really don’t respond at all to procedures. In the age of predictive analytics, we now have a lot of data from the past 10 years to help risk adjust what a patient’s chance of success may be.
The main factors we look at are the symptoms — what are they, are they classic, how many atypical features are present? The more atypical features, the more we start to question the diagnosis. We also look at the degree of vascular compression on the patient’s MRI. More severe compression has correlated with higher chance of success and long-term benefit. We look at whether it’s an artery or a vein that’s compressed. In general, the chance of success tends to be better with arterial compression than with venous compression. We consider whether the patient has had prior procedures that didn’t work. Each subsequent procedure, on average, tends to have a slightly lower chance of success. We also assess for any overlapping pain syndromes. If the patient also has occipital neuralgia or reflex sympathetic dystrophy, that raises the question of whether there may be a central component or central mechanism of the pain.
Advertisement
In other words, we try to think about all these different factors for any given patient, to help counsel them on what the chance of success is with a potential procedure. That’s needed because it’s very easy for patients to get information from the internet or from a relative with face pain that may not apply to them. It’s key to recognize that everyone’s pain is different and everyone’s situation is different.
Advertisement
Advertisement

Despite the condition’s debilitating, electric shock-like pain, treatment options are better than ever
A review of takeaways from the recent U.K. national guidelines

Routine capture of standardized neuroperformance data may expand and refine investigations

Reimagining the outpatient neurological visit with routine capture of neuroperformance data

Updates on this fast-evolving therapeutic landscape from a leading trialist

What the postoperative data show so far

Types and presentation may differ from adults, but early recognition and intervention are just as key

An expert talks through the benefits, limits and unresolved questions of an evolving technology