Locations:

Expert team helps 43-year-old woman regain quality of life
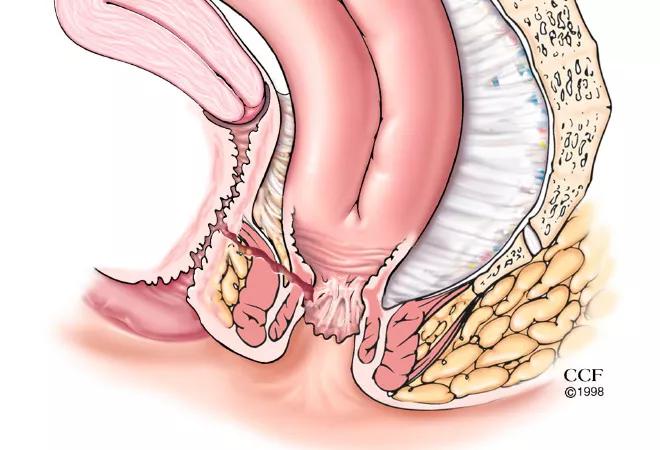
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/534fb28a-7da8-4d75-8b99-9d8192570925/17-DDI-009-Pouch-Vag-Fistula-CQD_jpg)
17-DDI-009-Pouch-Vag-Fistula-CQD
By Tracy Hull, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Cleveland Clinic performs the highest volume of inflammatory bowel disease surgery in the country, and has particular experience managing patients sent with complications after surgery elsewhere. Overall mortality and morbidity scores are exemplary based on recent NSQIP datasets, even allowing for the high percentage of reoperative surgery performed at this institution.
Vignette:
A 43-year-old woman from another state had ulcerative colitis diagnosed 10 years prior. When medical therapy no longer kept her symptoms under control, her colon had to be removed.
After removing her colon, surgeons had constructed a pelvic pouch from her small bowel, connected it to her anal area, and formed a loop ileostomy. Her hospital course after surgery lasted nearly two months, because she developed a failure of the joining between the pouch and her anal sphincter muscles. They had thought this had healed, but the leak became evident again when her ileostomy was closed. She next underwent a redo pouch and loop ileostomy, again in her home state. When the ileostomy was done at the time her second pelvic pouch was closed, she started to have stool and gas from her vagina (i.e., she had a hole between the pouch and the vagina).
At this stage, she came to Cleveland Clinic. While reviewing her outside records, we noted a concern from a gynecologist regarding cystic masses in her ovaries so she was seen in conjunction with a gynecologist at Cleveland Clinic. A combined surgery was then performed, with the colorectal surgeon and the gynecologist operating together. The gynecologist removed her uterus, tubes and ovaries while the colorectal surgeons did a third redo pouch and loop ileostomy.
Advertisement
The patient stayed in the hospital for seven days after the surgery. The loop ileostomy was closed in December 2014 and she remains with good bowel function, no holes and no vaginal drainage. She has been able to return to her job as a teacher.
References:
Advertisement
Advertisement

Landmark trial data suggest appendectomy may reduce relapse and improve remission rates in select patients

Implications for surgical decision-making and patient management

Dr. Prabhu discusses mentorship, collaboration and her vision for the future of the department

New program looks to innovative approaches for advancing early detection and multicancer prevention

Patients have a significantly higher risk of developing fistulas and experiencing future Crohn’s-like changes

Cleveland Clinic researchers developed an objective tool to assess response following total neoadjuvant therapy.

Patients may benefit from booster appointments, psychological support

Research demonstrates cirrhosis regression in one-third of patients, with higher rates using alternative assessment