Locations:

Retrospective looks at a “direct to angio” MSU strategy and mechanical thrombectomy beyond 24 hours
Timing is paramount in treating acute ischemic stroke, but nuanced questions around the timing of certain assessments and interventions remain. Researchers with Cleveland Clinic’s Cerebrovascular Center began to address two such questions in a pair of abstracts presented at the 2023 International Stroke Conference (ISC):
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Use of a mobile stroke unit (MSU) in management of suspected ischemic stroke is associated with improvements in thrombolytic delivery times and patient outcomes, as Cleveland Clinic and other early adopters of MSU therapy have reported. “We also have the ability to perform CT angiography in the MSU, which provides a further potential advantage,” notes Cleveland Clinic interventional neurologist Gabor Toth, MD.
To explore that potential, he and his Cerebrovascular Center colleagues conducted an initial analysis reported in one of the ISC abstracts. They performed a retrospective chart review of patients from 2014 to 2022 with acute ischemic stroke due to ELVO who arrived at Cleveland Clinic’s tertiary care comprehensive stroke center via MSU, comparing outcomes between those went to the angiography suite directly from the MSU (DTA group; n = 14) and those who first underwent additional imaging studies upon arrival to the hospital before going for angiography (CTA group; n = 52).
Compared with the CTA group, the DTA group was more likely to receive thrombolytic therapy (P = 0.03) and had shorter door-to-groin times (39 minutes for DTA vs. 51.5 minutes for CTA; P = 0.02).
However, recanalization was less successful with the DTA approach, with unfavorable Thrombolysis in Cerebral Infarction (TICI) grades of 0 to 2a seen in 35.7% of the DTA group compared with 9.6% of the CTA group (P = 0.03). And while the two groups achieved statistically comparable functional outcomes as assessed by modified Rankin Scale (mRS) score, the DTA group had higher mortality (35% vs. 9%; P = 0.028).
Advertisement
The two groups were comparable on demographic and clinical factors except for slightly but not significantly higher NIH Stroke Scale (NIHSS) scores in the DTA group and a higher rate of tandem occlusions in the DTA group. The latter difference may have swayed recanalization success and outcomes, Dr. Toth notes.
“In real-world practice, I would not expect mortality to be higher in the DTA group, unless these patients were sicker,” he says. He adds that, in addition to the possible impact of differing tandem occlusion rates, these results may be attributed to selection bias resulting from the study’s retrospective, nonrandomized nature and small sample size.
Dr. Toth emphasizes that these initial findings do not mean a direct-to-angiography approach in select patients may not make a positive difference in the right setting. “This small-scale study is a first step,” he says. “Hopefully larger prospective studies of a more systematic approach will follow, particularly on MSUs, to help identify which patients would benefit from going directly to angiography and which should have imaging in advance of thrombectomy. Regardless of these findings, MSUs continue to fit into our practice exceedingly well and shorten time to treatment.”
Mechanical thrombectomy (MT) has demonstrated benefits within 24 hours in acute ischemic stroke patients selected with advanced imaging in large studies. However, less is known about the safety and efficacy of MT beyond 24 hours after last known normal.
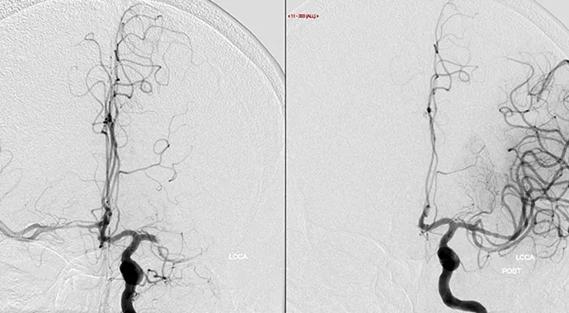
To help fill that knowledge gap, Cleveland Clinic staff reported at ISC 2023 on a retrospective analysis of 39 patients who met extended-window trial criteria but received MT beyond 24 hours. [Editor’s note: The study has since been published in full in Journal of the Neurological Sciences.] They found that clinical outcomes and safety were comparable to those observed in large trials of MT within 24 hours, especially in patients with anterior circulation occlusion.
Advertisement
Revascularization was successfully achieved in 87% of patients, with a median of two passes. Overall, 49% had a favorable outcome (95% CI, 34%-64%), and 95% were free of complications. The median improvement in NIHSS score from baseline to discharge was 3.0 (interquartile range, 1.5 to 8.0).
Patients had a median age of 69, and half (48.7%) had M1 segment occlusion. Three patients (7.7%) experienced symptomatic intracranial hemorrhage, which is in line with large studies conducted within the 24-hour window.
“Although the study was retrospective, the fact that there wasn’t a significant decline in successful outcomes or an increase in procedural complications or safety events, such as symptomatic intracranial hemorrhage, is an important finding,” notes Dr. Toth, a co-investigator on the analysis.
While the positive findings were not unexpected, he adds that presenting these results is important in view of the 24-hour time window for MT specified by current guidelines. “We know from prior studies that modern imaging technology can be safely used for patient selection, even in patients who present in the late time window,” he says. “Imaging assistance should help eliminate arbitrary time restrictions for acute stroke.”
Patients in the study discharged to a favorable discharge facility (home, home health or rehab) were much less likely to have a poor mRS score at 90 days (odds ratio = 0.11; P = 0.004). Notably, an exploratory analysis showed that having posterior circulation occlusion was associated with a poor mRS score (odds ratio = 14.7; P = 0.016). “Anterior circulation occlusion was associated with better outcomes than posterior circulation occlusion,” Dr. Toth notes, but he cautions that any conclusions must be limited, given the small number of patients with posterior circulation occlusion and the study’s retrospective design.
Advertisement
“We know that posterior circulation patients have symptoms that are much harder to diagnose, and these patients often present later, or are misdiagnosed, because of their atypical neurologic symptoms,” he explains. “Conversely, the natural history of posterior circulation strokes is known to be significantly worse, and this population would need more aggressive and effective treatment options.
“The question of thrombectomy beyond 24 hours is getting more and more attention, and I predict that more data will be coming out soon,” Dr. Toth concludes.
Advertisement
Advertisement

Aim is for use with clinician oversight to make screening safer and more efficient

Increasing treatment options are extending the window for continued functional gains
Study links large artery atherosclerosis and delayed presentation to poorer treatment results

$3.2 million grant will fund use of calcium-based imaging to record neuronal activity in ischemia model

Findings from large cohort analysis can guide ongoing quality improvement initiatives

Insights and what’s next for the first U.S. mobile stroke unit to treat patients

Research to test clinical efficacy and cost-effectiveness versus standard-of-care rehab

Times to target blood pressure, CT and medication administration shorter than with EMS transport