Locations:

How it’s similar but different from the direct anterior approach
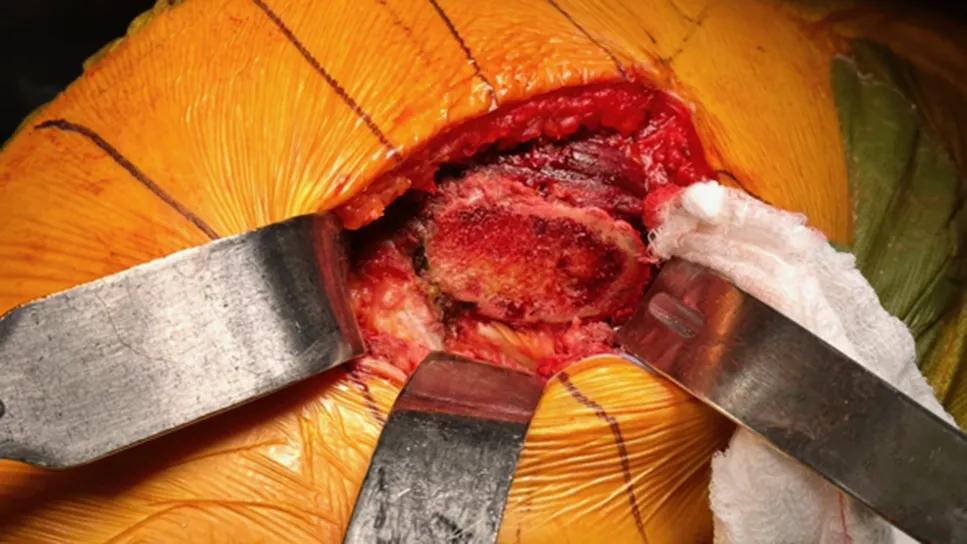
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cc6b8f86-5273-46b5-9ad9-c5754ce9aa07/anterior-based-muscle-sparing-hip-replacement)
Anterior-based muscle-sparing hip replacement
Anterior approaches to hip replacement continue to rise in popularity, offering alternatives to the conventional posterior and lateral approaches. Some patients perceive anterior approaches as preferable due to decreased muscle trauma and, therefore, quicker recovery — although Cleveland Clinic orthopaedic surgeon Nicholas Scarcella, MD, says there are benefits and limitations to every hip replacement approach.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In direct anterior hip replacement, the hip joint is accessed through the front of the groin, between the sartorius and tensor fasciae latae muscles. A newer, lesser-known approach is anterior-based muscle-sparing (ABMS) hip replacement, in which the hip is accessed between the tensor fasciae latae and gluteus medius.
“ABMS is one interval over from direct anterior, so some think it’s not a true anterior approach because it’s slightly lateral,” Dr. Scarcella says. “However, both ABMS and direct anterior approaches are anterior to the femur.”
While the ABMS name boasts muscle sparing, direct anterior hip replacement also avoids splitting or detaching muscles.
“ABMS has had several different names: anterolateral, ABLE [anterior-based muscle-sparing advanced lateral exposure] and modified Watson-Jones, among others,” Dr. Scarcella says. “In the past decade or so, ABMS has become the standard name, although it’s really no more muscle-sparing than a direct anterior surgery.”
In this Q&A, Dr. Scarcella explains more about ABMS, one of hip replacement’s newest surgical options.
A: I’m most comfortable with ABMS and have had the most experience with it because it’s how I was trained during my fellowship at Duke University Hospital. I think the approach any surgeon prefers typically depends on where and how they were trained. I also learned direct anterior and posterior approaches during my training.
A: ABMS is similar to direct anterior in that it improves stability compared to posterior and lateral approaches, which cut or detach major muscles. There’s less risk of dislocation after surgery. And, because there’s no muscle trauma, early stages of recovery are faster. Studies have shown that, three to six weeks after hip replacement, patients have less pain with anterior-based approaches compared with posterior or lateral approaches. However, one year after hip replacement, patients all do about the same, no matter the approach.
Advertisement
Compared with direct anterior surgery, ABMS surgery can be more extensile. The interval you’re in can be extended all the way down the leg and up the thigh for bigger exposure, if you run into problems. That can be an important factor in revision arthroplasty as well. In a hip revision, the ABMS approach allows me to access more of the femur and acetabulum without detaching muscles. That’s not necessarily true with the direct anterior approach.
A: Patients who are best suited for ABMS hip replacement tend to be younger, with more active lifestyles. The improved stability and quicker recovery are preferable for those who want to resume activities faster, including returning to work and recreation. Anterior hip approaches do not have as many postop restrictions as posterior hip approaches.
ABMS may not be best for patients with:
A: We use a standard operating table, like we do for a posterior or lateral approach. This is different from the direct anterior approach, where surgeons often use a specialized table, and patients are in supine position. For ABMS, patients are in lateral position.
Acetabular preparation is similar to what we do for a posterior or lateral approach. That can make ABMS more comfortable for surgeons who are used to doing conventional hip replacement procedures because they can visualize the acetabulum the same way.
Advertisement
Just as with other approaches, I can use robot assistance to place the acetabular component, ensuring high accuracy.
A: Compared with posterior and lateral approaches, anterior approaches have a slightly higher risk of wound issues, such as necrosis and infection. This is due to the incision’s proximity to the groin.
Risk of femoral nerve injury also is higher with anterior versus posterior or lateral approaches. However, the risk is lower for ABMS surgery than direct anterior surgery. With ABMS, the incision is one interval lateral to a direct anterior, so there is more muscle and soft tissue between the incision and femoral nerve.
Historically, femoral component loosening was slightly higher in anterior-based approaches. Now, with the advent of different femoral component and stem technologies, that is no longer a problem.
A: For the first two weeks, most patients use a walker and are fully weight bearing. There aren’t many precautions compared to a posterior approach, where patients can’t bend over and can’t internally rotate. Most patients transition to a cane at around two weeks and are walking independently around four weeks. They can drive three to four weeks after surgery. By six weeks, if pain and swelling aren’t a problem, I usually let patients return to all normal activities.
Advertisement
Advertisement

Study challenges assumptions about risk evaluation in total hip revision

Study highlights the need for objective functional measures as value-based care expands

Reduces likelihood of achieving CMS-defined substantial clinical benefit at one year

Should surgeons forgo posterior and lateral approaches?

Multidisciplinary care can make arthroplasty a safe option even for patients with low ejection fraction

High-risk procedure prepares patient for lifesaving heart surgery

Cleveland Clinic is among the first in the U.S. to perform the procedure

Insights to help orthopaedic practices comply with the 2025 CMS mandate