Locations:

Hybrid treatment model helps improve cancer care access

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c7f179af-7146-44f4-9823-0d8c13f7f71e/CNR_5153460_08-12-24_001_LDJ)
Dr. Pennell
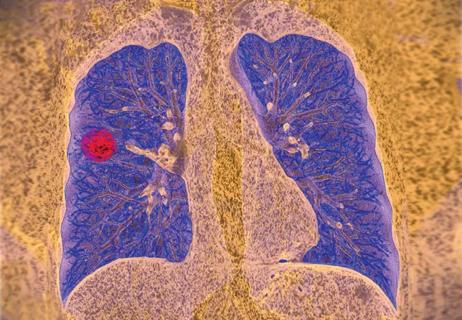
Until recently, there were few viable alternatives for treating small-cell lung cancer (SCLC). The primary first-line treatment is chemotherapy and checkpoint inhibitors such as durvalumab and atezolizumab. However, when patients progress, second-line therapy is not effective for most patients and does little to improve overall survival.
BiTE therapy called tarlatamab has replaced chemotherapy as second-line treatment. “This is probably the biggest advance in small cell lung cancer since the approval of immunotherapy," says Nathan Pennell, MD, PhD, co-director of the Cleveland Clinic Lung Cancer Program and Vice Chair of Clinical Research for Cleveland Clinic Cancer Institute. "It's a very exciting way to essentially deliver immune therapy that doesn't rely on the immune system to individually attack the cancer, which is how previous immune therapies tended to work."
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Tarlatamab is a bispecific antibody that binds to DLL3 (which is present in most SCLC) and CD3. The FDA granted accelerated approval for tarlatamab for previously treated SCLC, based on the international phase 2 trial DeLLphi-301. Two hundred twenty patients participated in the trial. Forty percent of those in the 10-mg cohort (97.5% CI, 29 to 52) and 32% of those in the 100-mg cohort (97.5% CI 21 to 44) achieved an objective response rate. Among those with an objective response, the duration of response was at least six months in 59% of patients. At the time of data cutoff, objective response continued for 22 of 40 patients in the 10-mg cohort and 16 out of 28 patients in the 100-mg cohort.
“It’s not just the response rate that’s promising but the duration of response,” says Dr. Pennell. “Second-line chemotherapies for small-cell lung cancer tend to only work for a few months. The average duration of response with BiTE therapy is more than six months, with one third of patients experiencing a response for more than nine months. "In the world of small-cell lung cancer, that's considered a fairly long duration of response.”
In the real-world setting, Dr. Pennell and his team administer a 10-milligram dose of tarlatamab. They’re seeing similar response rates in their patients to what occurred in the study.
Although many lung cancer therapies require a particular biomarker to be effective, that's not the case with tarlatamab since DLL3 is expressed in most SCLC patients.
Usually if a patient is relatively healthy and well enough to withstand treatment, has received one platinum-based chemotherapy as well as one other form of treatment, they are a candidate for BiTE therapy. However, to date there is no way to predict whether this therapy will work for a specific patient.
Advertisement
Due to the specialization involved with the treatment and management of side effects, BiTE therapy is currently only available at tertiary cancer centers like Cleveland Clinic Cancer Institute. In this setting, specialists bring deep experience in the administration and management of cell therapies.
For the first two rounds of treatment, patients are admitted to the hospital overnight for observation (and several days for treating side effects if they occur). If patients are tolerating side effects well, they can be observed for roughly eight hours on an outpatient basis for the third round of treatment. Once they complete this “ramp up” phase they can continue to receive subsequent infusions at the tertiary cancer center or return to whichever cancer center where they normally receive treatment.
The two major side effects of concern in BiTE therapy are:
• Cytokine release syndrome (CRS). This side effect occurs when the patient's body mistakenly believes the white blood cells that are attacking the cancer are due to an infection. "You get a situation that looks very much like sepsis or septic shock," explains Dr. Pennell. This includes fevers and low blood pressure.
Patients stay in the hospital to receive fluids to support their blood pressure and Tylenol for fevers. In more severe cases, clinicians administer tocilizumab, an antibody against the pro-inflammatory cytokine interleukin 6 (IL-6). This medication calms down the immune system. Fortunately, most patients do not experience CRS more than once. When it does happen, this adverse event occurs virtually immediately after initial therapy.
• Immune effector cell-associated neurotoxicity (ICANS). This adverse event is due to inflammation in the brain that can cause patients to become confused, weak or fall into a coma. It ICANS occurs, it tends to happen several weeks into treatment, although it may occur sooner. If a patient experiences ICANS, clinicians usually administer steroids to help suppress the inflammation. Patients can recover fully, and typically only experience this side effect once.
Advertisement
“Most of the time the adverse events are limited and treatable,” says Dr. Pennell. “The drug is extremely well tolerated and has few other side effects.”
In the DeLLphi-301 trial, CRS occurred in 51% of patients in the 10-mg cohort
and 61% of those in the 100-mg cohort. These were grade 1 or 2 in most cases. Three percent of patients had to stop therapy because of treatment-related toxicities. One patient in the 10-mg cohort passed away due to respiratory failure related to
treatment.
In the DeLLphi-301 trial, ICANS and related neurologic symptoms were observable in 11 patients (8%) in the 10-mg cohort and in 24 patients (28%) in the 100-mg cohort. In the 10-mg cohort, all incidents were grade 1 or 2. In the 100-mg cohort, 4 patients (5%) experienced grade 3 ICANS.
Patients benefit from having support from family and friends, especially early on in therapy. “It's important for caregivers to stay vigilant and call if their loved one is getting fevers, feeling lightheaded or is overly sleepy,” says Dr. Pennell.
“If you're suspicious that a patient may need to change therapy, seek a referral for BiTE therapy immediately. SCLC is extremely aggressive, and patients can go from feeling well to very sick in a short period of time.
The best time to consider second-line therapy is when scans have shown the cancer is no longer responding but before the patient has developed significant symptoms. That allows a bit of time to arrange the consultation and treatment. At Cleveland Clinic Cancer Institute, there is generally a one- to two-week waiting period for coordinating the initial inpatient stays.
Advertisement
Often patients don't want to or aren't able to travel to a city where they can safely access this treatment. If a patient faces a travel barrier for the initial therapy, they may potentially be able to receive care locally if their cancer center is comfortable doing so. In this case, Dr. Pennell recommends that their local oncologist talk with their own hospital pharmacists and hospitalists to determine if they’re comfortable carrying the medication on formulary and if they have experience managing cell therapy side effects like CRS and ICANS.
For now, reaching out and having a pipeline of communication to the lung cancer specialty team at your local tertiary care center can help expedite referrals. To that end, time-to-treatment is an important metric at Cleveland Clinic Cancer Institute. Typically, oncologists at the institute see patients within seven days of referral. However, that's not always possible at other tertiary cancer centers.
As more BiTE therapies become available and oncologists become more acclimated to managing patients in the hospital with these side effects, availability of the therapy will become more widespread.
In addition, the effectiveness of BiTE therapy is encouraging researchers to explore if it would be beneficial for newly diagnosed patients. There are clinical trials using tarlatamab in combination with chemotherapy and targeted treatments for SCLC in the frontline setting.
Advertisement
Advertisement

Treatment assigned FDA review date in June 2025

Cleveland Clinic, the University of Minnesota and University of Cambridge receive $1M grant to develop point-of-care biosensor for early detection and treatment personalization
Resection, radiotherapy or ablation?

Extent of baseline burden impacts progression-free and overall survival

Quantum computing being studied as a means to help improve predictive performance, accuracy

Young age, solid tumor, high uptake on PET and KRAS mutation signal risk, suggest need for lobectomy
Targeting DNMT1 shows promise in chemotherapy- and immunotherapy-resistant SCLC
New review published in Cancers suggests a synergistic benefit