Locations:

Treating a challenging cancer with novel use of radioembolization and SBRT
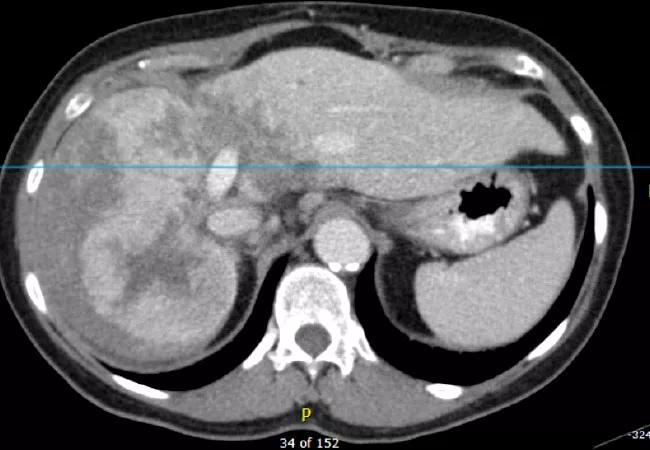
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e9e47a0e-d26f-4749-adef-753cf8612a07/19-CNR-4143-650x450-Liver_jpg)
19-CNR-4143 650×450-Liver
By Kevin Stephans, MD and Ihab Haddadin, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 69-year-old woman was diagnosed with a large hepatocellular carcinoma/cholangiocarcinoma. This mixed tumor, which measured 10 cm in the right lobe of the liver, extended across the midline to a portion of the left lobe. The liver had no cirrhosis and liver function was good.
Due to the extent of the disease, surgery was not an option. Because the tumor was a mixed type, chemotherapy was not advised.
This case was presented to a multidisciplinary liver tumor board, including specialists in hepatology, medical oncology, radiation oncology, surgery, radiology and interventional radiology. The board devised a novel two-pronged approach: radioembolization with yttrium-90 (y90) microspheres for the right lobe and stereotactic body radiotherapy (SBRT) for the left lobe.
The goal for the right lobe was maximum tumor regression. As such, an interventional radiologist injected tiny beads with high-dose y90 through the patient’s hepatic artery, which supplied the tumor. (The portal venous circulation, supplying the liver’s healthy tissue, was preferentially spared.)
y90 is ideal for hepatic radioembolization because of its relatively localized radiation emission with short penetration depth, limiting collateral dosing to nonembolized hepatic and extra-hepatic tissue. The y90 beads were distributed throughout the tumor’s right lobe, providing relatively comprehensive radiation to the right lobe portion of the tumor from the inside out over several days.
Unlike external beam radiation, radioembolization avoids entry and exit dosing concerns. Mapping the patient’s hepatic vasculature helped to minimize the number of radioactive beads deposited outside the tumor into healthy liver tissue.
Advertisement
Conventional direct imaging of the y90 radionuclide is not feasible, but positron emission tomography /computed tomography (PET/CT) imaging can quantify the distribution of y90 decay activity, thereby showing the technical success of radioembolization and helping predict its efficacy.
Following each y90 injection, the patient underwent a PET/CT scan to determine and direct repeat treatments. The patient ultimately had five y90 treatments and one bland embolization (intended to block the tumor’s blood supply without delivering radiation due to challenging anatomy).
Radioembolization was not used in the left lobe because of the risk of radioactive beads migrating downstream through the hepatic vasculature beyond the tumor into the healthy left liver, representing the majority of the patient’s hepatic reserve. To spare normal tissue and allow for residual liver function, SBRT was used instead. SBRT directs multiple radiation beams from various angles to intersect in a target area, allowing for accumulation of high radiation dose at the intersection of beams with more modest entry and exit doses.
An active breathing control system enabled the most precise SBRT treatment. With a snorkel-like apparatus placed in the patient’s mouth to monitor lung volume and temporarily pause inhalation and exhalation, active breathing control allows radiation to be delivered only at certain times in the respiratory cycle, when the patient’s tumor target is at a precise position. This helps counteract movement of the tumor when the patient breathes, allowing for a smaller target volume and thereby minimizing radiation dose to the patient’s heart and other non-targeted areas.
Advertisement
The patient received five treatments of SBRT with active breathing control, administered every other day, to reduce radiation impact on the bile duct.
The patient reported minimal to no radiotherapy-associated side effects such as fatigue and nausea. Upon treatment completion, she returned to Cleveland Clinic every three months for repeat imaging.
Although radioembolization was expected to destroy much of the patient’s right lobe, it showed ample regrowth with restored function. The tumor in the left lobe resolved completely. The spared distal portion of the left lobe demonstrated hypertrophy over time.
While the patient had an excellent response to treatment with minimal residual disease, she required further treatment for isolated focal recurrences. She was able to maintain an excellent quality of life, traveling throughout the world with her family for a period of time that exceeded her initial estimated survival of 6 to 18 months. Unfortunately, more than 4 years after initial presentation, she died secondary to an acute thrombosis of her left portal vein following a viral illness.
The large size and rare dual phenotype of this patient’s tumor made this an extremely challenging case. Rather than assuming there were no curative treatment options and referring the patient to hospice, Cleveland Clinic Cancer Center devised a unique two-pronged approach to reduce the tumor, resulting in an extended preservation of the patient’s functional capacity.
Radioembolization with y90 and SBRT with active breathing control each have discrete advantages. Combining the approaches allows a patient to achieve each treatment’s individual benefits. This innovative combination is not available in many cancer centers, given the relative novelty of each treatment and the need for careful multidisciplinary collaboration. At this time there are few scientific studies informing how to calculate radiation tolerance in combined radiotherapy. PET/CT imaging helped guide this case.
Advertisement
This case illustrates the benefits of multidisciplinary collaboration, especially among experts in interventional radiology and radiation oncology. Where individual radiation therapies fall short, combining them can offer new hope.
Dr. Stephans is a Cleveland Clinic Cancer Center radiation oncologist and Dr. Haddadin is an interventional radiologist.
Advertisement
Advertisement

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care

Research findings offer clues for improving disease outcomes in men

Creating a safe space for patients

Long-term immune effects reshape preventative strategies and timelines

Large-scale database also reveals potential for immunotherapy to protect against cancer

Findings may help guide discussions around prognosis and allogeneic stem cell transplantation