Locations:

Correction of nonunion restores function in an active adult
In early 2020, a 37-year-old man underwent a C5-C7 anterior neck fusion at an outside institution, after which he was initially symptom-free. Several months later, however, he began experiencing neck and arm pain, which led him to return to his surgeon that summer for a consultation. On reviewing postsurgical imaging, the surgeon told him the multilevel fusion was solid and nothing more could be done.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Over the next 18 months, the patient’s pain worsened and was accompanied by a choking sensation. As his symptoms progressed, the patient — a fit and active former gymnast — found he could no longer play with his 9-year-old son or perform day-to-day functions, and he fell into a depressed state.
Experiencing intractable pain and now unable work, the patient sought out a second opinion from Thomas Mroz, MD, a spine surgeon in Cleveland Clinic’s Center for Spine Health.
“This was a young man who had been very active, and his postsurgical pain had massive downstream consequences,” says Dr. Mroz. “His condition spiraled to the point that he had lost his livelihood, and his relationship with his son was suffering. Our evaluation showed that he had a nonunion at the C5-6 and C6-7 levels (Figure 1) and that he was a candidate for revision surgery.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/a67541bc-81c9-413c-8094-e4cfeff6a735/22-NEU-3097424-CQD-Inset1-800x458-2_jpg)
Figure 1. Preoperative X-ray (left) and CT (right) demonstrating nonunion.
Nonunion, or failure of solid fusion in the first year after cervical spine fusion, occurs in a fraction of patients who undergo such surgery. The risk of nonunion increases in proportion to the number of levels in the spine involved in a procedure. Some patients with a failed fusion are asymptomatic, but approximately 60% have progressive pain.
Imaging techniques used to diagnose nonunion are X-rays and CT scans. Diagnostic anesthetic injections are often very useful in helping confirm the nonunion as the source of the patient’s pain. Once a nonunion occurs, the likelihood of union with any nonoperative modality is very low. Surgical procedures include repeat anterior and/or posterior instrumented fusion.
Advertisement
The key to success when treating post-spine surgery patients who have pain, according to Dr. Mroz, is individualizing the approach in keeping with patients’ particular symptoms and condition. “We take an algorithmic approach to understand what is bothering the patient and carefully review imaging to determine whether the origin of the pain is something simple, like a loose screw, or if more structures are involved,” he explains.
To try to confirm the nonunion diagnosis, an anesthetic facet injection was performed that relieved the patient’s pain. Once the diagnosis was confirmed, Dr. Mroz and the patient had an in-depth discussion about the benefits and risks of a revision operation, which resulted in a decision to proceed with the surgery.
Dr. Mroz performed a revision anterior neck fusion at the C5-6 and C6-7 levels. Rather than leaving any of the original hardware, he removed and replaced it to maximize the likelihood of proper fusion and ensure mobility (Figure 2).
“Sometimes when we do revisions, we come in from the back,” says Dr. Mroz. “But given that this patient was a very active former athlete, we decided to go from the front and take everything out and revise the fusion.”
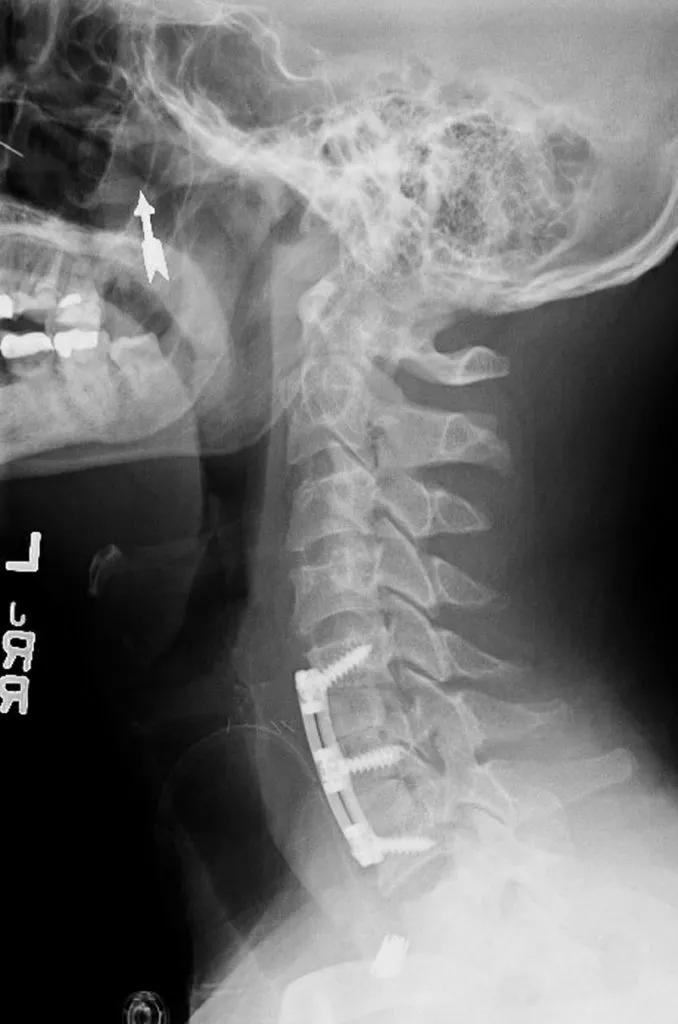
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/8f245344-5ff5-4fae-b915-8c3d71b231a4/22-NEU-3097424-CQD-Inset2-800x1209-2-678x1024_jpg)
Figure 2. Postoperative X-ray demonstrating the revision fusion at C5-6 and C6-7.
When the patient was seen for follow-up less than two months after the surgery, “he reported no pain and said he walked 130 miles and lost 15 pounds since the surgery,” says Dr. Mroz. “His sensation of choking was gone, and he said he feels ‘awesome’ and is spending more time with his son.”
The key takeaway from this case, according to Dr. Mroz, is for clinicians to be open to seeking referrals for patients who have chronic pain after spinal surgery. At the Center for Spine Health, care is available from a multidisciplinary team that includes spine surgeons, medical spine and pain specialists, and other professionals who specialize in spine care.
Advertisement
“Primary care physicians may not have the tools to evaluate these individuals properly,” Dr. Mroz says, “and it is understandable that some surgeons may not be comfortable doing revisions. But patients who have chronic postsurgical pain should be made aware of all the treatment options available.”
Advertisement
Advertisement

Findings may have implications for understanding the disorders’ pathophysiology

Routine capture of standardized neuroperformance data may expand and refine investigations

Nearly one-fifth of such cases fulfill 2024 McDonald criteria based on biomarkers

Adequate dosing may improve outcomes in well-selected patients, large Cleveland Clinic series suggests

Reimagining the outpatient neurological visit with routine capture of neuroperformance data

Free portal helps researchers classify and share data using the IC-CoDE framework

Large study shows rural patients are less apt to be discharged to inpatient rehab, hampering outcomes

Updates on this fast-evolving therapeutic landscape from a leading trialist