Locations:

A brief history

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6d4f5dbf-b869-4747-8c1c-0bf503cbf266/freezing-fat-cells-jpg)
Fat cells
by Shannon Wu, Demeterius M Coombs, MD, and Raffi Gurunaian, MD, PhD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
*Note: This is an abridged version of an article originally published in the Cleveland Clinic Journal of Medicine. For the full article, please click here.
Liposuction is the second most commonly performed cosmetic surgery in the United States and the most common surgical procedure in patients between the ages of 35 and 64.1 Practitioners of medicine and surgery will undoubtedly encounter these patients in their practice. This brief review discusses the role of liposuction and fat transfer in aesthetic and reconstructive surgery, as well as indications.
In 2018, surgeons performed 258,558 liposuction procedures, a 5% increase from 2017.2 The number of liposuction procedures increased 124% from 1997 to 2015.3
Liposuction is advantageous in that the removal of fat cells limits future deposition of fat in those areas.4 Ultimately, liposuction allows plastic surgeons to semipermanently redistribute volume in accordance with a patient’s ideal, and with lower complication, morbidity and mortality rates than with other surgical procedures. In addition to its utility for purely aesthetic purposes, liposuction is an important adjunct in reconstructive surgery, particularly of the breast and face, when harvested fat is autologously reinjected in these tissues. One particular procedure rising in popularity and gaining significant attention in the media is gluteal fat grafting.
The first attempt at fat removal was by Dujarrier in 1921, who operated on the knees and calves of a dancer. Injury to the femoral artery led to amputation of the leg.5 In 1964, Schrudde curetted subcutaneous fat from a patient’s leg, but observed skin necrosis in four of 15 separate patients, in addition to hematoma and seroma.6
Advertisement
The era of modern liposuction began in 1975 when Arpad and Fischer pioneered the use of blunt hollow cannulas and suction curettage for liposuction on the outer thighs, but the patients ultimately experienced deforming lymphorrhea.7 An important milestone was reached in 1977 when Illouz developed the “wet technique,” in which injection of hypotonic saline solution and hyaluronidase into adipose tissue before liposuction reduced hemorrhagic risk.8 This type of hydrodissection, similar to that used today, preserved neurovascular bundles and enlarged the deep adipose layer for easier aspiration.
In 1983, Fournier used syringes instead of mechanical suction for better control of negative pressure.9 By 1987, Klein had developed the tumescent technique—a type of local anesthesia infiltration that permitted the removal of larger volumes of fat while reducing bleeding.10 Toledo expanded the use of syringes to include various gauges and sizes for aspiration of adipose tissue in 1988.1
In the early 1990s, the development of ultrasonographically guided liposuction by Zocchi expanded the use of liposuction for previously unfavorable, fibrous areas such as the buttocks.12,13 The development of minimally invasive, laser-assisted liposuction by Apfelberg, also in 1992, prevented destruction of neurovascular structures by cannulas and promoted tissue tightening for an aesthetic result.14 Recently, the development of power-assisted liposuction has further expanded and improved this procedure, increasing the popularity and use of liposuction.15
Advertisement
Liposuction is used to achieve body contouring by removing excess fat deposits in undesirable areas of the body. Fat is suctioned from demarcated areas in the body amenable to contouring. The most common area for fat removal is between the inframammary fold and gluteal fold—namely, the abdomen, flanks, trochanteric region, lumbar region, and gluteal region (Figure 1). Other areas of fat removal include the breasts (e.g., breast reduction surgery), thighs and calves. The site of incision is an important anatomic consideration, and the surgeon should select regions where the surgical scar, although modest, can be hidden by clothing, as well as locations conducive to broad fanning of the cannula during the procedure.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/14505c1c-765e-4bd6-a1ac-3d11c8d92f78/20-PSX-1953078_Inset_F1_large_805x840_jpg)
Figure 1. Left: Preoperative appearance of a 52-year-old man who presented for liposuction of localized adiposity within the abdomen and bilateral flanks. Right: The same patient 6 months later after removal of 1.4 L of adipose tissue.
There are five zones in which superficial subcutaneous tissues adhere to underlying deep fascia of muscle: the lateral gluteal depression, gluteal crease, distal posterior thigh, midmedial thigh and inferolateral iliotibial tract. Because these zones define the natural shape of the body, suctioning from these areas increases the risk of contour deformities.16 Ideally, patients have adequate skin elasticity and are within 20% to 30% of their ideal body weight to achieve desired aesthetic outcomes.17
Liposuction is also increasingly being used as an adjunct to enhance other aesthetic procedures such as breast augmentation, cervicoplasty, abdominoplasty, gluteal fat transfer and body contouring for postsurgical bariatric patients (Figures 2 and 3).18 Liposuction can also be used to promote gender-specific features.19 In women, the goals of liposuction are to promote shapely contours of the breasts, waist, hip and buttocks. In men, liposuction aims to achieve upper body dominance, such as removing excess flank adipose tissue (“love handles”).
Advertisement
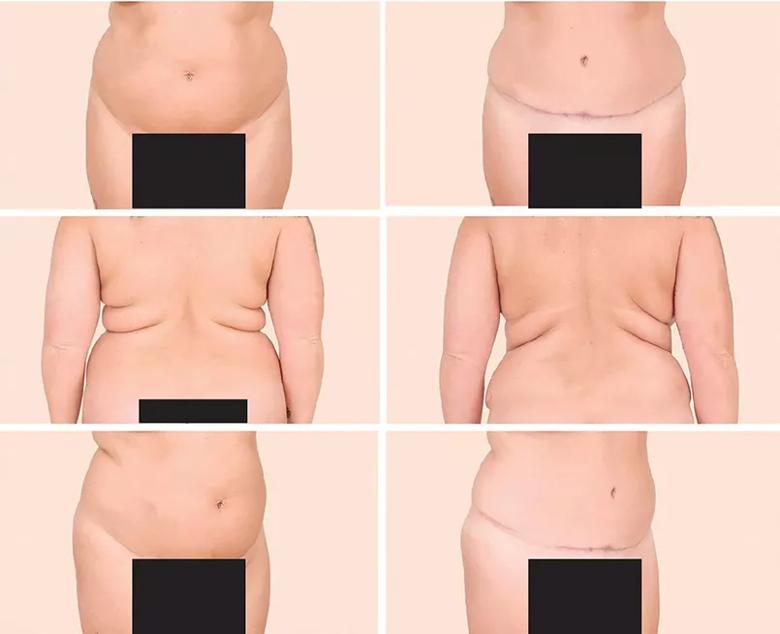
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/0e3b207a-3d76-4e82-bd10-2cd171f49f53/20-PSX-1953078_Inset_F2_large_805x654_jpg)
Figure 2. Left: A 38-year-old woman who presented with excess skin and adiposity of the anterior abdomen and excess adipose tissue in the bilateral upper back and hips. Right: The same patient 5 months later after full cosmetic abdominoplasty and liposuction of the bilateral upper back and hip areas (with a total of 2 L of tissue removed), illustrating that these procedures may be combined safely and yield satisfying results.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/99382a81-5276-4aaf-a1a1-8da383af52b9/20-PSX-1953078_Inset_F3_large_805x455_jpg)
Figure 3. The same patient from Figure 2, now almost 19 months after surgery but having lost weight, demonstrating stable long-term results after abdominoplasty and liposuction. Note the stable improvement in bilateral flank and upper-back adiposity.
Gluteal fat transfer, popularly called the “Brazilian butt lift,” is an application of liposuction in which large volumes of fat are transferred from an undesirable area, such as the abdomen or inner thighs, to the buttocks.20 Fat is first removed by liposuction (the volume of which varies widely and remains largely based upon the patient’s preoperative anatomy) and is then used to augment the contour of the buttocks commensurate with the patient’s desires and anatomic deficiencies.21,22
High-volume fat transfer, defined as a volume greater than 1,000 mL per buttock, has historically been associated with a higher risk of infection at the graft site and seroma formation at the harvested site. Newer evidence suggests high-volume buttock fat transfer may be safe and effective with proper technique.23
Thus, the contour is improved in both the donor region, such as the waist, and the recipient region. The popularity of gluteal fat transfer is rapidly increasing due to shifting beauty standards in American culture and attention from celebrity figures. More than 26,000 gluteal fat transfer procedures were performed in 2018, a 16% increase from the previous year, and a 132% increase from 2013.3,24 However, reports of fatal pulmonary fat embolisms following injury to gluteal veins and an estimated mortality rate of 1 in 3,000 from this procedure warrant continued investigation about its safety and ideal technique.25
Advertisement
The Multi-Society Gluteal Fat Grafting Task Force26 was established to investigate and improve patient safety of this procedure, and current research including anatomic studies as well as educational symposia are ongoing. Risks and alternative methods such as gluteal implants must be discussed with the patient before this procedure. Moreover, as with any aesthetic or reconstructive procedure, the American Society of Plastic Surgeons recommends that patients seek consultation from a board-certified plastic surgeon.
Liposuction is also being used for reconstructive purposes, including management of the following disorders:
Additionally, liposuction can be used to:
Although no absolute contraindications exist for liposuction, relative contraindications should be considered during the patient evaluation.31 Anticoagulants and medications that interfere with lidocaine metabolism should be stopped before liposuction.32 Poor skin firmness and elasticity in elderly patients would lead to poor skin draping postoperatively and potentially increase patient dissatisfaction.
Further, reasonable expectations must be established, and patients with body dysmorphic disorder may require a psychiatric consultation before surgery. Patients with diabetes mellitus, cardiac disease and liver disease may need medical clearance before surgery at the discretion of both the surgeon and the facility where the procedure is to take place. Lastly, as has been discussed elsewhere in the surgical literature, poorly controlled diabetes increases the risk of infection.
To view the reference list, please click here.
Advertisement

Family history may eclipse sun exposure in some cases

Consider secondary syphilis in the differential of annular lesions

Persistent rectal pain leads to diffuse pustules

Two cases — both tremendously different in their level of complexity — illustrate the core principles of nasal reconstruction
Stress and immunosuppression can trigger reactivation of latent virus

Low-dose, monitored prescription therapy demonstrates success

Antioxidants, barrier-enhancing agents can improve thinning hair

A hybrid approach