Locations:

Why and how we’re using robotic assistance for qualifying CABG candidates
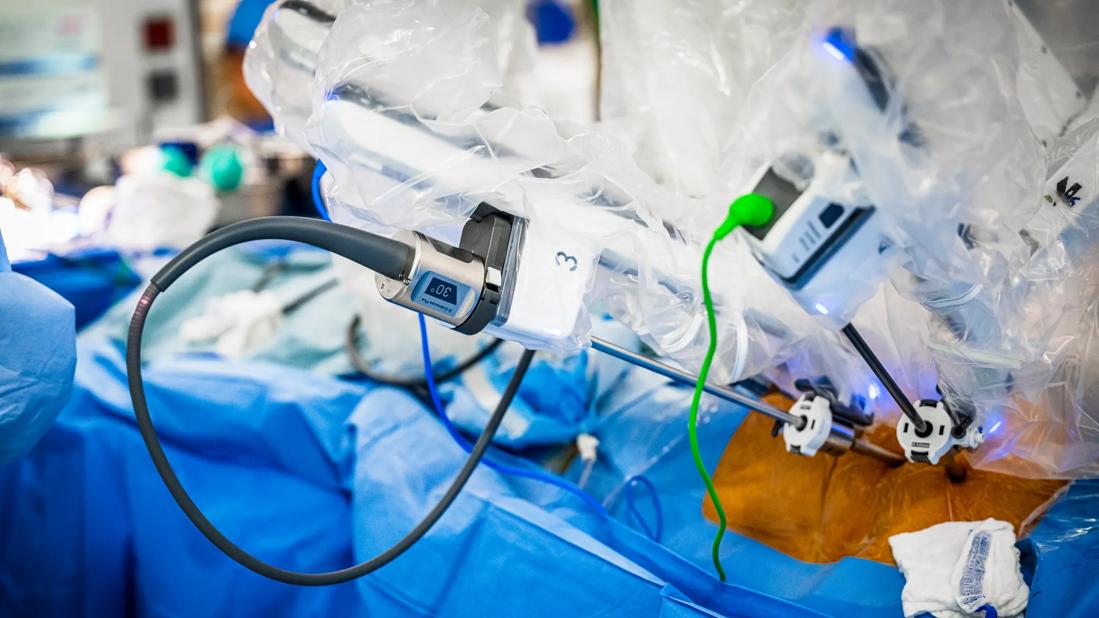
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2f5b9854-804c-4f43-8f7a-70dc239303f5/HVI_5240459_09-26-24_018_SCG)
robotic arm ports in a cardiac surgery operation
The LIMA-LAD graft (left internal mammary artery to left anterior descending artery) is considered the holy grail of coronary artery bypass graft surgery (CABG), due to its durability and proven ability to improve survival. Cleveland Clinic cardiac surgeons now offer minimally invasive, robotically assisted LIMA-LAD grafting to patients who qualify.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Avoidance of sternotomy is the major difference between robotically assisted CABG and standard CABG,” says Donna Kimmaliardjuk, MD, who co-directs Cleveland Clinic’s robotic CABG program with colleague Faisal Bakaeen, MD. “This is a far less invasive procedure, with just a small incision made between the ribs.
“In terms of outcomes,” she continues, “robotically assisted CABG is very safe, and patients get a great bypass. The advantage is in its faster recovery time. It’s far easier to recover from a 2- to 3-inch thoracotomy than from a sternotomy. Patients can return to their usual activities, including work and sports, much faster.”
Cleveland Clinic surgeons started doing robotically assisted coronary artery bypass more than a decade ago, but they found the approach and technology were not sufficiently advanced to make the procedure as safe and effective as conventional CABG. Both the technology and patient selection criteria have since improved within the framework of a rigorous process and a dedicated team approach, so Cleveland Clinic relaunched its robotically assisted CABG offerings earlier this year.
Currently, only single-vessel bypasses are performed with robotic assistance. Dr. Kimmaliardjuk expects that will change. “Our goal is to develop the ability to do double- or triple-vessel bypasses through a small incision,” she says.
The ideal candidates for robotic CABG are those needing only a single LIMA-LAD bypass. For those with blockages in other arteries that are amenable to stenting, the option of a hybrid procedure is available. The hybrid procedure is done in conjunction with interventional cardiologists.
Advertisement
“We have shown that using arteries to bypass all important target vessels improves survival,” says Dr. Bakaeen, Director of Cleveland Clinic’s Coronary Artery Bypass Surgery Center. “However, using arteries to bypass less-important vessels will not necessarily increase survival. These vessels can be stented.”
“The ability to offer patients the holy grail of a LIMA-LAD bypass without a traditional full sternotomy has significant implications for the future of coronary revascularization,” adds interventional cardiologist Khaled Ziada, MD. “Interventional cardiologists and cardiac surgeons can ‘map out’ a plan to give patients the best of both worlds: second- and third-generation stents for non-LAD lesions, which compare favorably with vein grafts, and a mammary bypass for the LAD, which has traditionally been superior to stenting in this territory. Clinical trials will need to establish the potential advantages of this approach in the near future.”
Robotic technology has increased the pool of candidates who receive a LIMA-LAD graft to certain populations who are regularly excluded due to technical challenges. These include patients with obesity.
“The beauty of robotic surgery is that it allows us to harvest a mammary artery of sufficient length to reach the target and even bypass more distal disease,” Dr. Bakaeen notes. “Additionally, better visualization makes harvesting the artery less traumatic.”
Interventional cardiologists generally serve as gatekeepers to robotic CABG, identifying potential candidates based on angiography. The surgeons review the pros and cons of conventional versus robotic approaches with the candidates and cardiologists.
Advertisement
“We arrive at what we feel is the best option for a given patient,” Dr. Kimmaliardjuk explains, “taking into account how many vessels need to be bypassed, the patient’s overall health, the presence of comorbidities, and the patient’s ultimate goals and expectations for quality of life and longevity.”
Technical criteria for robotic CABG include:
It is not necessary for patients to have a usable conduit other than an IMA, since bilateral internal mammary artery grafting is not performed, and radial arteries are not used.
The goal of robotic CABG is to provide a LIMA-LAD graft equal in quality and durability to that achieved with a sternotomy.
“The LIMA-LAD graft is the most important thing we can do for a patient with coronary artery disease,” Dr. Bakaeen observes. “In younger patients with LAD disease, robotically assisted MIDCAB [minimally invasive direct coronary artery bypass] can provide a lifetime solution.”
“We never want to compromise quality or safety for the sake of cosmesis,” Dr. Kimmaliardjuk notes. “If we have any concern for the patient’s safety or the quality of the bypass during the surgery, we can convert to sternotomy.”
Advertisement
Quality is enhanced by careful patient selection and perfect execution. “We assess graft flow in the operating room as a form of quality control, and we verify graft patency before closing,” Dr. Bakaeen says. “We do not accept results that are less than perfect.”
Safety is secured by the high level of expertise across the multidisciplinary team involved in the care of these patients, including cardiologists, cardiac anesthesiologists and intensivists. “As surgeons, we play an important, but only partial, role in the total experience,” Dr. Kimmaliardjuk says.
“As interventional cardiologists, we work very closely with our surgical colleagues to provide each patient with an individualized heart team approach,” adds Laura Young, MD, of the Section of Interventional Cardiology. “With the recent advancements in robotic CABG, we can offer more patients a hybrid approach of stenting and bypass surgery to provide the most optimal, durable results with the least invasiveness.”
“We are excited about this program,” Dr. Kimmaliardjuk says. “It is young, but we have achieved excellent results. To date, all LIMA-LAD grafts remain open, and there have been no conversions to sternotomy.”
“Cleveland Clinic has consistently received a three-star rating for CABG from the Society of Thoracic Surgeons (STS), and its operative mortality rate for isolated CABG has been less than half the rate predicted by the STS risk model for many consecutive years,” notes Dr. Bakaeen. “It is with this emphasis on quality and excellence that we have relaunched the robotic CABG program for the benefit of patients.”
Advertisement
Advertisement

After four decades, refinements to the gold standard of bypass continue as new insights emerge

BITA grafts themselves are rarely to blame, and outcomes can be good

Two cardiac surgeons explain Cleveland Clinic’s philosophy of maximizing arterial graft use

Cleveland Clinic-pioneered repair technique restores a 61-year-old to energetic activity

Study indicates lower in-hospital mortality and better long-term survival

How Cleveland Clinic supported an alliance hospital to improve early extubation practices

Findings undercut perceptions of radial artery as second conduit of choice

CMR-CLIP outperforms general AI tools; may one day expand patient access to CMR