Locations:

Suspected factors include antithrombotic intensity, time on device, presence of thrombocytopenia
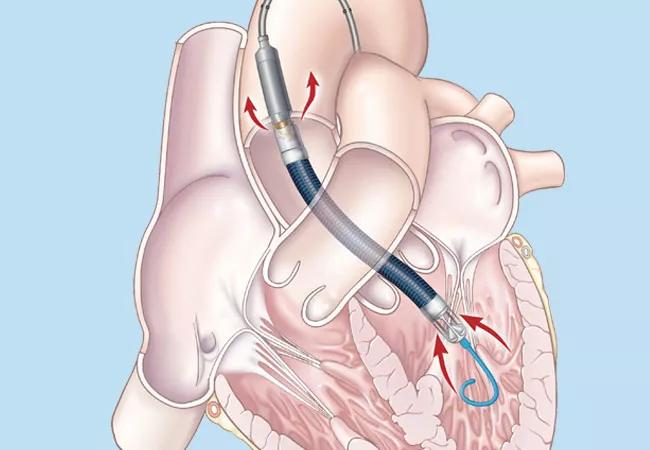
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9fb56661-d60f-47b1-ada0-6961668c350d/20-NEU-1951118_Impella-temporary-LVAD_650x450_-1_jpg)
20-NEU-1951118_Impella-temporary-LVAD_650x450_ (1)
For patients on short-term cardiac support with an Impella device, inadequate anticoagulation, duration of cardiac support and a low platelet count all may play roles in causing an ischemic stroke or intracranial hemorrhage. So finds a newly published single-institution series from Cleveland Clinic (ASAIO J. 2020;66[8]:e105-e109) analyzing outcomes among 79 patients with acute cardiogenic shock who underwent implantation of Impella, a percutaneously placed temporary left ventricular assist device (LVAD).
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Ischemic stroke and intracranial hemorrhage are common causes of death and disability in patients who receive a long-term implantable LVAD, with many of these events occurring perioperatively. But the incidence of, and risk factors for, acute neurologic events in patients on short-term cardiac support with a percutaneous temporary LVAD have not been well characterized.
“Causes of these devastating acute neurologic events with short-term Impella support have not been thoroughly explored,” says stroke neurologist Ken Uchino, MD, the study’s senior and corresponding author and Head of Research and Education in Cleveland Clinic’s Cerebrovascular Center. “Our case series revealed plausible risk factors and sets the stage for further investigation.”
Dr. Uchino and colleagues reviewed prospectively collected data on 79 consecutive patients implanted with an Impella device (Impella 2.5, 5.0, CP or RP) at Cleveland Clinic between October 2010 and July 2018. The median duration of Impella support was 8 days (range, 1-33).
Six patients (7.5%) were found to have had an acute neurologic event, as follows:
Of these six patients, four died during hospitalization, and the other two survived to heart transplantation (one underwent transplant the day before the acute neurologic event). Analysis of the six patients revealed the following:
Advertisement
The incidence of ischemic or hemorrhagic stroke in this series (7.5%) was higher than in other published studies, which found a less than 2% incidence during the implantation period. The researchers note that while the reasons for this difference cannot be answered by this study, their findings focus attention on several key questions:
Advertisement
“This small retrospective study cannot determine the exact cause of neurologic events in Impella-treated cardiogenic shock patients, a population with a high risk of stroke and many confounding factors,” concludes Dr. Uchino. “But it does highlight a number of issues that will be helpful to explore in larger randomized controlled trials and prospective studies.”
Advertisement
Advertisement

How to use? Consider starting during the acute attack and seek patient preferences for chronic use

Quantitative imaging adds diagnostic value beyond 3T MRI in nearly half of patients

Expert shares insight on intrathecal baclofen pumps to treat spasticity

Opportunities and impacts of a growing surgical approach

Despite safety concerns and mixed trial results, experts see potential for this indication

Experts endorse a push to improve prevention and treatment following repetitive head injury

A population with very high lifetime risk presents care challenges and pathophysiologic insights

Two Cleveland Clinic neurologists review biomarker advances, targeted therapies and unresolved clinical challenges