Locations:

A principal investigator of the landmark longitudinal study shares interesting observations to date

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/fb32aa77-0d6e-47c6-8761-d7de3a9be3c9/brain-study-first-three-years)
woman in red shirt standing beside a sign for clinical study recruitment
Three years have passed since the launch of the Cleveland Clinic Brain Study in early 2022. In that time, the first-of-kind longitudinal study has enrolled more than 3,600 adult volunteers with no known neurological disease to undergo regular comprehensive assessments designed to detect biomarkers and causes of neurological disorders before symptoms manifest.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The effort is similar to what the landmark Framingham Heart Study set out to do in the late 1940s, except with a focus on neurological disorders instead of cardiovascular disease — and with the support of the latest imaging and diagnostic technology.
“The goal of the Cleveland Clinic Brain Study is to identify new biomarkers and targets for preventing or curing neurodegenerative and other neurological disorders, with the aim of enabling disease detection and intervention as early as possible,” says Imad Najm, MD, who serves as the study’s co-principal investigator along with Andre Machado, MD, PhD, Chief of Cleveland Clinic Neurological Institute.
Consult QD caught up with Dr. Najm for an update on the study’s enrollment as well as initial findings, surprises and next steps. An edited transcript of the interview follows.
Dr. Najm: Eligible volunteers are adults with no known neurologic disease who are 50 or older. That age threshold is lowered to 20 or older for individuals who have a first-degree relative with multiple sclerosis. Participants complete quality-of-life questionnaires every six months and are assessed annually for many measures and every two or five years for others. Assessments include structural components such as brain and retina imaging, cognitive components such as neuropsychological exams, and neurophysiological components such as EEGs and sleep studies. We also perform blood and stool testing to evaluate potential systemic and microbiome indicators of neurologic risk.
Advertisement
Dr. Najm: Robust. Approximately 12,000 people have expressed interest by registering on the study website. Several thousands of volunteers did not meet the inclusion criteria or decided they weren’t able to commit to what’s involved, which leaves over 3,600 individuals who have completed at least one annual assessment plus another 2,000 or so individuals who qualify and have scheduled or are waiting to schedule their first assessment.
Of the 3,600-plus volunteers who have begun the study, nearly 1,000 have completed two visits and nearly 500 have completed three visits. The study has an attrition rate of approximately 8% per year, which compares very favorably with the typical attrition rate of about 20% per year reported for similar studies. The volunteers so far have been very excited to participate.
Dr. Najm: The mean age of the 3,600-plus enrollees is approximately 67 years, with 60- to 65-year-olds making up the largest five-year age cohort. Enrollees range in age from 50 to over 90. Enrollees so far have been nearly 75% female and over 85% white, with 6% of enrollees being black, 2% Hispanic/Latino, <1% Asian, <1% Native American and 4% declining to report their race/ethnicity. As neurodegenerative and other neurological disorders can impact anyone, we are working to increase participation to better reflect our entire population.
Enrollees have come from 46 of the 50 U.S. states. About two-thirds had previously been Cleveland Clinic patients.
Dr. Najm: The most surprising finding is how neurologically healthy this population has been. This may be due in part to the self-selection involved in participating in a study like this, where people who are health-conscious and engaged may be more apt to volunteer. Whatever the reason, we have not detected much evidence of neurological disease among the first 3,600-plus enrollees. For instance, we have not discovered a single case of Parkinson’s disease, Alzheimer’s disease or epilepsy in any of our volunteers during their first year of testing.
Advertisement
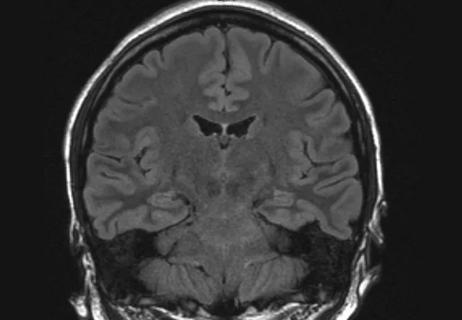
We have found a few silent strokes. These are small strokes seen on MRI that did not cause any clinical problems in speech, sensation or motor function. The volunteers were unaware that they happened. We have also seen a small number of volunteers — less than 1% — showing demyelination or other myelin problems. We have referred these patients for thorough clinical assessment.
Dr. Najm: It’s important to note that, at this stage of the study, we are not looking closely at every single study result, such as sleep studies. Based on the studies we are looking at, the leading incidental finding has been brain aneurysm, which we have seen in slightly more than 120 volunteers, both on MRI and on MR angiogram. In fact, this is the first known study that has examined the incidence of brain aneurysms in a healthy population using MR angiogram. This rate is a little higher than the traditionally reported 1% to 2% incidence of brain aneurysms in the general population. We also see that the incidence of brain aneurysms seems to be increasing with age.
These are interesting findings and are the subject of a manuscript our neuroradiologists are preparing. When we detect one of these aneurysms, we alert the volunteer and advise them to seek follow-up care with their physician of choice, sharing the digital imaging findings.
The second most common incidental finding on MRI is low-grade brain tumors, mostly meningiomas. We also have found a much smaller number of low-grade neck tumors. Additionally, we are seeing a fair amount of white matter disease, which is not surprising in a population of this age. In many cases it is not significant; if it is more widespread or suggestive of demyelination or multiple sclerosis, we refer for evaluation. Notably, we also discovered one tragic case of Creutzfeldt-Jakob disease before any symptoms developed.
Advertisement
Dr. Najm: These come from the periodic health questionnaires as well as from standardized neuropsychological and cognitive tests. Based on those results, we are seeing fairly high prevalences of depression, anxiety and possible sleep problems, particularly sleep apnea. The rates are not higher than would be expected in the general population, but they are among volunteers who are not aware they have these conditions.
On the cognitive front, we are seeing some enrollees who are very near the borderline for cognitive impairment. Now that we are a few years into the study, we are hearing from some of our brain health neurologists that a few of their newer patients with mild cognitive impairment are coming from the Brain Study. As expected, among our three-year participants, we are seeing some enrollees with a decline in cognition from year 1 to year 3.
Dr. Najm: Not many, but we have introduced a few additional assessments, such as a speech and language study involving voice digitization for analysis for early signs of neurodegenerative disorders such as Parkinson’s or Alzheimer’s disease. We also introduced a smell test. We are seeing quite a few volunteers with problems on the smell test, but none of them have yet shown parkinsonian features. Some of the smell issues may be due to COVID-19 infection, although some may signal a risk of Parkinson’s disease. We will have to see over time.
We are collecting a wealth of data that we are not yet analyzing, but additional data analyses are gradually getting underway. For instance, we are starting to look at brain connectivity based on functional imaging from study volunteers. We also are looking at scalp EEG findings. There are indications that findings from some of these electrodes can predict whether a volunteer is on the lower end of the range for normal cognition or is a “super ager.” The data are still preliminary, but this is one example of many fascinating avenues of research we are beginning to pursue.
Advertisement
Dr. Najm: We currently have six manuscripts planned or in the works that should be submitted for publication within the coming year. They will address the following:
Dr. Najm: We are pursuing NIH grant submissions to specifically support our analyses into cognitive and imaging findings from this study. We are also expanding our assessment infrastructure in Northeast Ohio with a new fully dedicated space for Brain Study testing, including a new 3T MRI machine with the most advanced clinical and technological capabilities. That space will be operational in the first quarter of 2026 and will allow us to nearly double our enrollment capacity.
Beyond those near-term developments, I am excited about the potential for many longer-term developments we can’t even predict at this point. We are collecting so much information and so many biosamples in this study — such as the ongoing blood and stool samples — that as our participants develop non-neurological diseases over time, I suspect our colleagues in other specialties are going to be very interested in analyzing our samples and longitudinal data for insights in their disciplines as well. This has the potential to be a very significant research endeavor across many specialties and disease areas.
Advertisement

Phase 3 STELLAR trial underscores role of molecular stratification in glioma care
GFAP elevation may signal increased risk of progressive regional atrophy, cognitive decline

Preclinical work promises large-scale data with minimal bias to inform development of clinical tests
Research aims to extend observations of reversal learning in mice to human neurological disorders

Multicenter collaboration aims to facilitate tracking of neurological activity deep within tissue
Diagnosis and treatment of MOG antibody-associated disease

Designed for digitization, distance health, discovery and more

Model of viral encephalomyelitis shows links with CNS recovery from inflammation and damage