Locations:

Making sense of the fast-moving treatment landscape
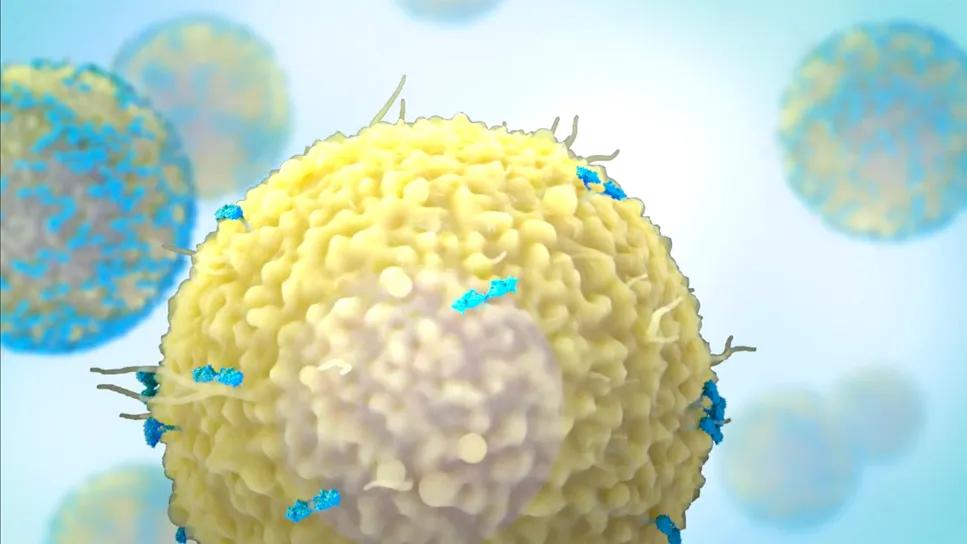
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c91c9da5-c2b4-4d21-9e74-18a1a4b393d1/car-t-and-bispecific-research-trials)
CAR T cell
Years ago, clinicians had few options beyond melphalan and steroids to treat multiple myeloma. Today, that situation has changed substantially, with new therapy approvals coming fast and furious.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The four-drug regimen of daratumumab, bortezomib, lenalidomide and dexamethasone in the frontline setting is greatly reducing the chance of early relapse. And with advances in CAR T-cell and bispecific therapies, patients are living longer and having improved quality of life.
“There are new ways to attack myeloma,” says hematologist/oncologist Shahzad Raza, MD. “CAR T-cell treatment is one of the best therapies that science has produced. Imagine a patient who has been on multiple myeloma therapy on a regular basis for years, and they can now have a treatment-free holiday and long-lasting disease control for several months or even years. That's very exciting for these patients.”
To date, there are two CAR T-cell therapies FDA approved for treating multiple myeloma:
Advertisement
Although there is no head-to-head comparison between the two types of CAR T-cell products, real-world analysis recently published in the Journal of Clinical Oncology showed superior efficacy and survival of cilta-cel, with higher incidence of certain toxicities compared with ide-cel.
Video content: This video is available to watch online.
View video online (https://cdnapisec.kaltura.com/p/2207941/sp/220794100/playManifest/entryId/1_tyk7ree3/flavorId/1_5f3sgelj/format/url/protocol/https/a.mp4)
There is an unmet need for access to these treatments outside of large academic centers. “The good news about CAR T-cell therapy is that it's a one-time treatment, so there's a definitive period of time the patient needs to be away from home,” says hematologist/oncologist Sandra Mazzoni, DO.
Patients usually receive CAR T-cell therapy in the hospital so they can be monitored for side effects, such as cytokine release syndrome. As the immune system is revved up, this can create an inflammatory “storm,” resulting in fevers, tachycardia, hypotension or neurological issues. If this occurs, clinicians administer the interleukin-6 inhibitor tocilizumab to reverse the side effects.
“The neurotoxicity profile resolves with time, but there are very rare circumstances with the cilta-cel product where some of those toxicities could cause weakness or other long-term changes neurologically,” says Dr. Mazzoni. “In the last two to three years, we’ve learned more about how to mitigate and manage these toxicities,” says Dr. Raza.
Time-to-treatment remains a challenge, however. Currently, it takes between six to eight weeks for CAR T-cell products to be manufactured and administered. Patients require bridging therapy in the meantime while they wait for their CAR T cells.
Advertisement
BiTE therapy works along a similar concept to CAR T-cell therapy. It stimulates and enriches the patient’s own T-cells and directs them toward destroying myeloma cells.
There are two FDA-approved BCMA BiTE therapies, teclistamab and elrenatumab, both of which are highly effective in the management of RRMM.
Another bispecific, talquetamab, targets GPRC5D (a protein that is highly expressed on multiple myeloma cells) is also FDA approved for management of RRMM.
BiTE therapies are administered subcutaneously during a ramp up period where dosing is titrated. Patients have a hospital stay (typically four to nine days) to be monitored for toxicities. The infection risk is also high with BiTE therapies, particularly with those that target BCMA. Patients who receive BiTE therapies should receive vaccinations and immunoglobins as a preventative measure. If side effects occur, the medication can be paused while a dose adjustment is made. Usually, side effects are grade one or two.
After the titrate and monitoring period is over, BiTE therapy is given on an outpatient basis. BCMA products are given weekly, while the CPRC5D product is given every two weeks.
BiTE therapy is mostly offered at large academic centers, which can be a barrier for patients who live far away. Only an estimated 20-30 percent of patients live within two hours of a center that’s qualified to administer bispecifics.
To improve access, Cleveland Clinic Cancer Institute partners with community practitioners. The patient stays inpatient at Cleveland Clinic during the initial step up and monitoring. If the patient lives far from Cleveland, the team can transition them back to their community oncologist to continue treatment once they’re discharged from the hospital.
Advertisement
Researchers are well under way in developing a host of additional multiple myeloma treatments, including:
Another area of interest is precision oncology. By integrating artificial intelligence and gene mapping with outcome and adverse event data, researchers hope to personalize treatment of multiple myeloma.
"BCMA CAR T-cell therapies and BiTE therapies have shown dramatic improvements in multiple myeloma outcomes,” says Dr. Raza. “The results were so powerful that we're starting to use these therapies much earlier in the disease course via clinical trial. CAR T-cell therapies are also given even in patients who are lenalidomide refractory.”
Refer patients while they’re still stable. It’s best to refer patients earlier in the disease course when they still have good disease control with their first-line treatment to allow time to plan. “This is especially true of patients with high-risk disease or who are not responding to standard induction therapy,” says Dr. Raza. “Sometimes relapses happen quickly. There are some patients who may not survive the wait for autologous CAR T-cell therapy if they have very active disease. Don’t wait until their performance status declines.”
Advertisement
Many patients who are not transplant eligible can receive CAR T-cell therapy. Even some patients in their 80s with reasonable performance status can potentially receive CAR T-cell therapy.
There is considerable real-world data about the performance of cell therapies in different populations. Cleveland Clinic published numerous studies1 about the use of cell therapies in various groups, including those with relapsed/refractory disease.
Consider clinical trials earlier in the patient’s cancer journey. Referring patients to an academic center can give them access to advanced treatments that are not yet commercially available.
As the therapeutic landscape moves forward, there are still many questions researchers are striving to answer to improve clinical care. Cleveland Clinic Cancer Institute is leading studies tackling larger questions, such as:
• Can CAR T-cell therapy take the place of stem cell transplant in the upfront setting?
• Is BiTE therapy appropriate in earlier lines of treatment?
• Would administering maintenance therapy after CAR T-cell therapy extend the duration of remission?
• Could combining bispecifics together give patients with aggressive disease a more sustained response?
1
https://pubmed.ncbi.nlm.nih.gov/39177290/
https://pubmed.ncbi.nlm.nih.gov/39632797/
https://pubmed.ncbi.nlm.nih.gov/38151105/
Hear our recent podcast about advancing treatment for multiple myeloma.
Advertisement

The shifting role of cell therapy and steroids in the relapsed/refractory setting

Phase 2 study brings pivotal advances in treatment efficacy and safety for the most challenging-to-treat population

Explaining common misconceptions about chimeric antigen receptor therapy

Clinicians share practices to streamline initiation of care

Prediction and bioinformatic data could prove valuable for therapeutic interventions targeting this malignancy

Findings from large database important to inform clinical practice

Study of 401,576 patients reveals differences in cancer burdens as well as overall survival
Despite sicker patients, response rates of teclistamab in a real-world study were similar to those from a pivotal clinical trial