Locations:


Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/d7f0af2d-65b1-47a2-9514-5121849376f9/overactive-bladder-2240867562)
Older patient with UTI
Editor’s note: This article originally appeared in the Cleveland Clinic Journal of Medicine.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
By Ellen K. Kendall and Yael Mauer, MD, MPH
Patients with symptoms consistent with urinary tract infection (UTI) do not need to be tested and should be treated.
Patients with classical UTI symptoms that include new or acutely worsening dysuria, urinary frequency, urgency, suprapubic pain, and hematuria, particularly in the absence of vaginal symptoms, can be diagnosed and treated for UTI without the need of urine studies. The probability of UTI is approximately 50% in women with any one of these symptoms and greater than 90% in women with dysuria and frequency without vaginal symptoms.1
When patients present with symptoms that are suggestive but not clearly diagnostic of UTI, urine studies should be obtained. Together with symptoms, the presence of bacteria, leukocyte esterase or white blood cells, nitrites, and hemoglobin or red blood cells in the urine support the diagnosis of UTI and its treatment.2
Patients with nonspecific findings such as malaise, altered mental status, and cloudy or malodorous urine, should not routinely be evaluated or treated for UTI, unless these acutely occur in patients with spinal cord injury or cognitive disability in which case urine studies are appropriate as the patient is unable to clearly express or experience classic UTI symptoms.2,3
Screening and treatment for asymptomatic bacteriuria, or bacteria in the urine without symptoms, should only be done in patients who are pregnant or preparing for a procedure associated with urologic mucosal trauma.3−5 If a positive urinalysis or culture happens to be obtained in any other patient, antibiotics should not be prescribed, as this can lead to possible side effects from treatment, antimicrobial resistance, and undue financial burden.3,5,6
Advertisement
UTI is very common in US adults.7,8 Prevalence in the overall population is approximately 11%, with increased prevalence (20%) in women over age 65.7 In the outpatient setting, around 15% of antibiotic prescriptions are for UTI.8
UTI refers to the presence of bacteria in the urine combined with symptoms, and UTIs are classified according to the location of bacteria in the urinary tract.7,9 The term simple cystitis refers to an infection of the lower urinary tract (bladder and urethra), with patients typically presenting with acute or worsening dysuria, urinary frequency and urgency, suprapubic pain, and hematuria.1,7,9 Complicated UTI, or pyelonephritis, refers to UTI that has extended to the upper urinary tract (ureters and kidneys) and usually presents with symptoms of systemic illness, such as fever, malaise, nausea or vomiting, and new or worsening flank pain.7,9
In men presenting with pelvic or perineal pain or voiding difficulties, prostatitis should be considered.10 Urethritis, typically caused by sexually transmitted pathogens, must be considered in sexually active men presenting with dysuria, pruritus, burning, or discharge at the urethral meatus.11
In postmenopausal women, chronic urinary frequency, urgency, or dysuria, especially in combination with vaginal symptoms, should prompt the clinician to consider genitourinary syndrome of menopause as opposed to UTI.12
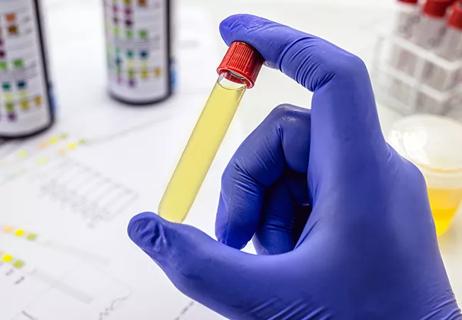
When a patient presents with atypical urinary symptoms and thus the diagnosis is unclear, urinalysis is recommended (either by dipstick or microscopy).
Advertisement
Dipstick testing evaluates for presence of leukocyte esterase, hemoglobin, and nitrites in the urine. Positive leukocyte esterase suggests the presence of pyuria or white blood cells.13–15 Hemoglobin is suggestive of red blood cells in the urine. Nitrites are highly specific for infection with Enterobacteriaceae, the most common organism responsible for UTIs, but because not all bacteria reduce nitrates, a negative test does not exclude infection.13
Dipstick urinalysis provides quick semiquantitative results and is usually performed in emergency and ambulatory settings. However, it is dependent on bacterial and cellular concentrations and thus often lacks sensitivity. The presence of nitrates or leukocyte esterase plus hemoglobin, has been shown to have a sensitivity of 77% and specificity of 70% for UTI in female patients, with positive predictive value of 81% and negative predictive value of 65%.14 The positive predictive value increases to 92% if nitrites plus blood or leukocyte esterase are present. The negative predictive value increases to 73% if all three are negative.14 In males aged 60 years and older, dipstick findings have been reported to have a positive predictive value of 83% and a negative predictive value of 60%.15
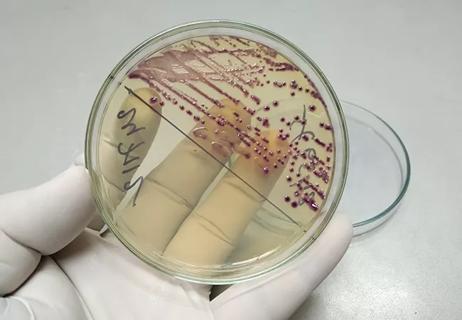
Urine microscopy examines urinary sediment and can most accurately detect and quantify cells in the urine, as well as identify casts, crystals, and pathogens.16-18 It can confirm findings on a dipstick or detect abnormalities missed by chemical testing, providing additional clues toward different diagnoses. For example, white blood cell casts are formed in the kidneys and thus suggest pyelonephritis rather than simple cystitis.
Advertisement
Urine culture can help guide antibiotic therapy in patients with pyelonephritis or cystitis that has failed empiric therapy, as well as in a number of other settings, such as pregnancy, compromised immunity, urologic abnormalities, presence of an indwelling catheter, stay in an inpatient healthcare facility, recent antibiotic use, or history of prior infection with antibiotic resistant urinary pathogens.17–20
Asymptomatic bacteriuria is characterized by bacteria in the urine without UTI symptoms, representing bacterial colonization instead of infection and is distinct from UTI.4 Thus, the term asymptomatic UTI is incorrect and should be avoided.
Screening for bacteriuria in asymptomatic patients is only recommended if a patient is pregnant (B recommendation, fair evidence) or will undergo a procedure that involves urologic mucosal trauma (strong recommendation, moderate-quality evidence).3,4 Although urine testing is frequently done for screening purposes in populations such as the elderly, those with indwelling catheters, and during perioperative management, evidence suggests that screening in these populations can lead to harm.3,5,21 If a positive urine test has been obtained in these populations, the patient should not be treated with antibiotics.3,5,6,20
According to the 2019 Infectious Diseases Society of America Asymptomatic Bacteriuria Screening Guidelines,3 the following populations should be screened:
Advertisement
The following should not be screened:
There is insufficient evidence to recommend for or against screening in the following:
For older patients without urinary symptoms or systemic signs of infection who present with acute mental status change, other causes should be assessed first, and supportive treatment is recommended over screening for UTI and subsequent antimicrobial treatment (very low-quality evidence).3 In a study of emergency room patients age 65 and older, the presence of altered mental status, malaise, or lethargy did not increase probability of bacterial infection.22
Currently, there is only anecdotal evidence demonstrating benefit of antibiotic treatment in patients with altered mental status and asymptomatic bacteriuria.23 In a recent study, antibiotic treatment was administered to 82.7% of 2,733 hospitalized adults (median age, 77 years) with asymptomatic bacteriuria, defined as a positive urine culture without symptoms attributable to UTI.24 Patients who were older, had altered mental status, or abnormal urinalysis were more likely to receive antibiotics. Antibiotic treatment was not associated with improved clinical outcomes, but rather with 37% longer hospital length of stay.24
Screening asymptomatic patients or those with nonspecific symptoms not consistent with UTI often leads to the discovery of asymptomatic bacteriuria for which treatment is usually not required. Inappropriate screening and treatment of UTI is costly to the individual, healthcare system, and society.25–27 A US study analyzing preoperative urinalysis data from 2007 to 2017 found that total spending on inappropriate preoperative urinalysis was $48,675,408, and the estimated cost for antibiotics following inappropriate urinalysis added an additional $4,854,109.25
Improper treatment of asymptomatic bacteriuria can also lead to antibiotic-associated complications, such as Clostridioides difficile infections, ototoxicity, hepatic necrosis, Stevens-Johnson syndrome, anaphylaxis, and increased antibiotic resistance.5,26 Data from a 2012 US retrospective analysis of female outpatient urine cultures noted Escherichia coli antibiotic resistance to ciprofloxacin to be 11.8% among all patients and 29.1% among those age 65 and older. Resistance to trimethoprim-sulfamethoxazole was as high as 22.2% across all age groups and 26.7% in those 65 and older.27 Rates of resistance are even higher in certain parts of the United States and continue to increase.
Treatment of UTI is always recommended when patients present with classical UTI urologic symptoms. In this case, urine studies are not needed to establish diagnosis.
Urine studies should be attained when patients present with symptoms that are not clearly diagnostic of UTI. In this case, the presence of bacteria, white or red blood cells in the urine supports treatment.2
Patients with nonspecific findings not consistent with UTI should not routinely be evaluated or treated for UTI unless they have mental or physical disability that precludes them from experiencing or expressing urologic symptoms.3
Asymptomatic patients should not be screened for or treated for asymptomatic bacteriuria unless the patient is pregnant or preparing for a procedure associated with urologic mucosal trauma.
Disclosures
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
References
Advertisement

How this technology is improving antibiotic use and stewardship
Up to 3 days faster than waiting for urine culture results

Revolutionizing pediatric urology with a new, less invasive approach
Study highlights benefits of nephrologist-led urine sediment analysis

New research highlights serious risks and the critical need for earlier advance care planning

Initiatives focus on the physical and emotional well-being of geriatric patients and their caregivers

Researchers explore the mental and physical benefits of social prescribing