Locations:

Study highlights benefits of nephrologist-led urine sediment analysis

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e4eaf82d-110b-4a41-95b0-4605d98294c0/23-URL-3687299-CQD-650x450-4_jpg)
urine bottle held by healthcare professionals with latex glove, toxicology test
Automated urine technology has become a popular choice for urinalysis microscopy. But findings from a new Cleveland Clinic-led study that compare its accuracy to that of a nephrologist-interpreted microscopy call its utility for diagnosing acute kidney injury (AKI) into question.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Owing to higher patient volumes and workflow standardization, nephrologist-performed microscopy has become more of a rarity in most healthcare centers in recent years, explains nephrologist Georges Nakhoul, MD, senior author of the study.
The drawback, however, is that laboratory-performed microscopy, which often relies on automated urine flow cytometry or digital imaging systems, lacks a trained nephrologist’s perspective, particularly when developing a differential diagnosis for AKI.
“The lab technicians don’t have the clinical information that we have when looking at a urine sediment, and they may miss findings that are relevant to the diagnosis,” explains Dr. Nakhoul. This led the team to compare both types of urine sediment analysis. They reported their findings in Kidney360.
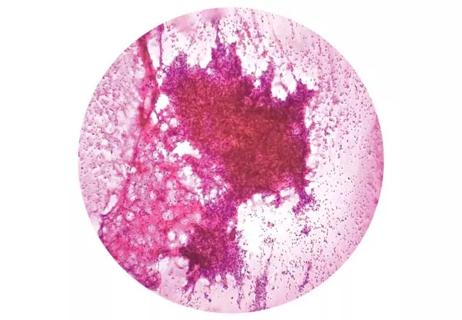
In the retrospective study, the team identified 387 Cleveland Clinic electronic health records of patients with AKI that contained laboratory-led urine sediment analysis (UrSA) and nephrologist-led UrSA completed within 72 hours of each other. The endpoints included the number of red (RBCs) and white blood cells (WBCs) per high power field, the presence and type of urinary casts per low power field, and the presence of dysmorphic RBCs.
The study found that automated processes can reliably quantify blood cells and squamous epithelial cells, and this finding is consistent with the literature. However, the study suggested that the lab analysis will often miss the presence of clinically relevant non-hyaline casts (such as muddy brown or RBC casts) and dysmorphic RBCs. For example, dysmorphic RBCs were detected in 18 instances on the nephrologist-led UrSA versus none on the lab UrSA.
Advertisement
“Our takeaway from the results is that many relevant findings to an AKI diagnosis were overlooked by the lab tests, including muddy brown casts that indicate acute tubular necrosis, dysmorphic red blood cells, or red blood cell casts. The lab evaluation captured none of these, which is notable because those are key diagnostic information when evaluating patients with acute kidney injury,” says Dr. Nakhoul.
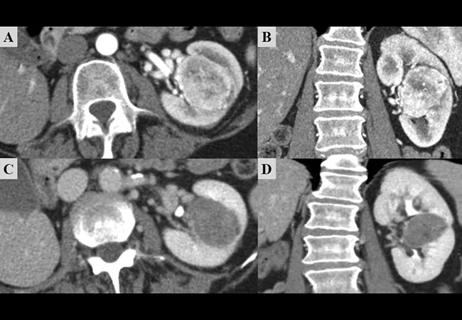
In a separate analysis of just the nephrologist-led UrSA, the research team then identified 33 patients with a kidney biopsy within 30 days of the nephrologist-led UrSA. They classified the sediment findings into four categories: bland, suggestive of acute tubular injury (ATI), suggestive of glomerulonephritis (GN) and suggestive of acute interstitial nephritis (AIN). The team then assessed agreement between both diagnoses.
In 90% of all the cases, the nephrologist-led UrSA reflected an accurate diagnosis based on the biopsy. Specificity was particularly high in the agreement between nephrologist-led UrSA and kidney biopsy in the ATI and GN cohorts, which is important when considering the necessity of a kidney biopsy in patients with relative contraindications.
While urine sediment examinations are one piece of the diagnostic puzzle in kidney disease management, they play an important role in informing clinical decision-making about medical management, including a kidney biopsy.
Dr. Nakhoul encourages other nephrologists to continue advocating for nephrologist-led UrSAs, particularly when approaching a differential diagnosis for acute kidney injury. “It’s time and cost-efficient and provides valuable clinical information. Our hope is that it continues to be part of training programs and also within the clinical practice of nephrologists.”
Advertisement
Advertisement

One pediatric urologist’s quest to improve the status quo

First single-port renal vein transposition reduces recovery time and improves outcomes
Fully-automated process uses preop CT, baseline GFR to estimate post-nephrectomy renal function
Belzutifan superior to everolimus in phase 3 clinical trial
Management of high-risk RMSK in the pre-and current eras of neoadjuvant therapy
NIH-funded study explores novel MRI technique to stage cystic kidney disease

AI-generated model bests predictive abilities of human experts

Using sequencing data to identify novel factors linked to kidney disease with unknown origin