Locations:

Novel approaches are available for patients at all stages of coronary artery disease
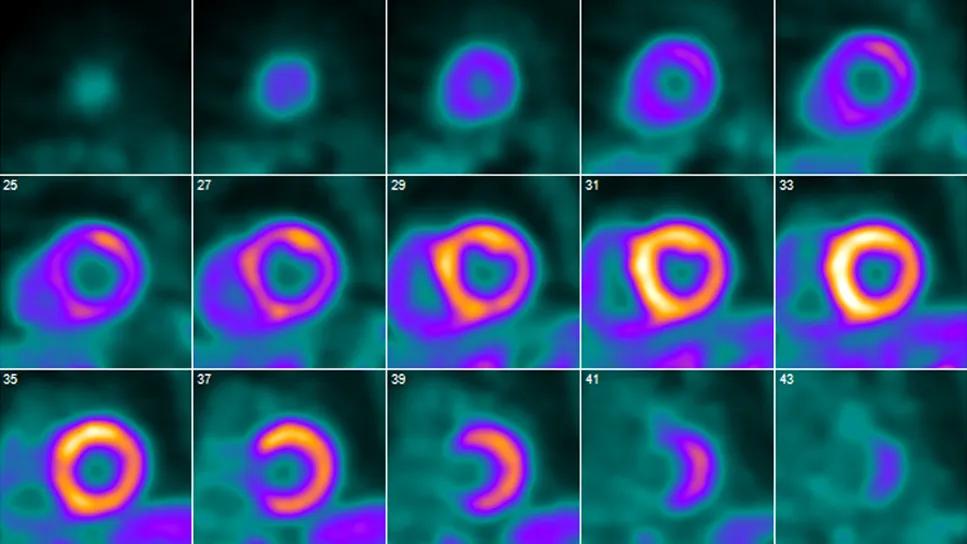
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7d3c9781-132a-431f-9bc5-58144ee19ff5/cardiac-PET-scan-feature)
series of cardiac pet scans
To many patients and clinicians, seeking out expert care for coronary artery disease (CAD) brings to mind referral for coronary artery bypass graft surgery (CABG) in cases of challenging anatomy or when a minimally invasive approach is desired.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Yet an innovative, high-volume heart program like Cleveland Clinic’s can offer patients with CAD distinctive care options at all stages of disease, including long before they may need revascularization. “Our Heart, Vascular & Thoracic Institute takes a comprehensive and highly integrated approach to CAD,” says Samir Kapadia, MD, Chair of Cardiovascular Medicine. “We have standout expertise in helping patients prevent or ameliorate various forms of CAD and advising them on the very best timing and method of intervention.”
This article is the first in a three-part series presenting a few selected examples of such expertise. This part focuses on noninvasive functional testing for obstructive CAD. Part 2 focuses on the management of a couple of special patient populations, and part 3 addresses refinements in revascularization care.
Because stress imaging offers greater sensitivity than exercise ECG testing alone, it is advantageous for diagnostic confirmation in many patients with symptoms suggestive of obstructive CAD. “Although stress testing is well established, it is not done equivalently everywhere,” says Wael Jaber, MD, a cardiologist in the Section of Cardiovascular Imaging.
A key consideration is volume-based experience, which looms large in stress echocardiography. At its Main Campus and family health centers in Northeast Ohio alone, Cleveland Clinic performs approximately 550 stress echo tests each month — about 500 with exercise and 50 with dobutamine. Most are done to evaluate for known or suspected CAD, although valvular heart disease, cardiomyopathy and metabolic stress testing are growing indications.
Advertisement
A leading advantage of stress echo testing is its safety and freedom from ionizing radiation. “Stress echo has been performed since the late 1970s, so there’s a wealth of diagnostic data as well as prognostic/outcomes data with long-term follow-up,” says Patrick Collier, MD, PhD, a cardiologist in the Section of Cardiovascular Imaging.
Patients with intermediate probability of CAD are most likely to have their management altered by the results of stress testing, Dr. Collier notes. Among stress testing options, stress echo is known to have relatively high specificity (a low false-positive rate). “Most experienced physicians will choose stress echo for their intermediate-risk patients who they deem less likely to have ischemia,” he says, “as such patients are more likely to have a true negative test in this context.” Because of changes in referral patterns, stress echo results that are “positive for ischemia” are less common, he adds, which poses challenges for both training and reporting.
“Stress echo testing requires deep experience on the part of sonographers and readers,” Dr. Collier says. “It’s important for patients and referring physicians to ensure that such testing is done at an accredited, experienced echo lab that performs a high volume. At Cleveland Clinic, we pride ourselves on the expertise of our sonographers (which is crucially important, as with all ultrasound-based tests) and the depth of knowledge and training of our physician readers, who stand out in terms of volume and experience. This is all the more important with the healthcare workforce challenges everyone has seen in the post-COVID era.”
Advertisement
For patients in whom radionuclide myocardial perfusion imaging (i.e., nuclear stress testing) is indicated, a center’s depth and breadth of technological capabilities is key, says Dr. Jaber, who has a specialty interest in nuclear imaging.
SPECT is the most widespread imaging modality for both exercise and pharmacologic nuclear stress testing, but it is limited by artifacts, which can lead to false-positive results in up to 30% or 40% of cases. To overcome this limitation, Cleveland Clinic is one of a small number of centers that perform CT attenuation correction on SPECT images.
“Ours is the only U.S. heart center that does CT attenuation correction on all our SPECT images,” Dr. Jaber says. “This enables us to remove many of the artifacts and improve image accuracy exponentially. This, in turn, reduces false-positive results and can spare patients the risk of unnecessary downstream testing.”
In addition to SPECT, Cleveland Clinic offers PET imaging for nuclear stress testing. Dr. Jaber says that while SPECT is a good choice for patients who prefer treadmill exercise over pharmacologic stress, and for those whose insurance doesn’t cover PET (which is more expensive), PET is a more advanced imaging modality that offers several advantages over SPECT:
Advertisement
The latter feature — blood flow measurement — is an important advantage. “Not only can we measure whether blood is getting to the heart, we can measure how much is getting there,” Dr. Jaber explains. “Without flow measurement, the sensitivity of traditional SPECT or PET is about 70% to 85%. When you add flow measurement, sensitivity improves to 95% to 98%. It’s rare for PET to miss a problem when flow measurement is performed.”
As a result, every PET stress test at Cleveland Clinic is done with flow measurement. And because Cleveland Clinic Main Campus has three PET scanners dedicated solely to cardiovascular cases, it performs 15 to 19 PET stress tests every day. “This is the largest single-center volume anywhere in the country,” Dr. Jaber notes. “At most other major institutions, cardiologists borrow PET cameras from their oncology departments to do stress tests, which means they can do only a handful per week, resulting in long wait times. We have virtually no wait time here.”

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/9bef09f3-1c62-4620-8f48-b183d336c40b/cardiac-PET-scan-inset2)
PET imaging for assessment of myocardial hibernation in a patient with obstructive CAD. Because it has three PET scanners dedicated to cardiac care, Cleveland Clinic is able to perform 15 to 19 PET stress tests daily.
Patients benefit from these advanced PET capabilities via greater diagnostic certainty as well as reduced radiation exposure and shorter testing time compared with SPECT.
PET with flow measurement also enhances the ability to guide revascularization. One example is through evaluation of myocardial viability, specifically with assessment of myocardial hibernation. “This enables us to determine, before any revascularization procedure, whether a section of heart wall that’s not moving is capable of recovery even with restored blood flow,” Dr. Jaber explains. “This allows us to spare patients the risk, pain and cost of having a procedure that may not benefit them.
Advertisement
“For all these reasons,” he says, “contemporary patients who need nuclear stress testing are best advised to go to a center that can readily offer PET to ensure the most comprehensive evaluation.”
Coronary CT angiography (CTA) is an increasingly used noninvasive imaging technique that plays a significant role in the assessment and management of CAD. It differs from stress testing in that it directly visualizes the coronary arteries and can quantify the extent of stenosis and assess plaque characteristics. In the latest multisociety chest pain guidelines, coronary CTA carries a class 1 indication for assessment of symptomatic patients with stable chest pain.
At Cleveland Clinic, coronary CTA currently plays a multitude of roles in CAD management for appropriate patients, according to cardiologist Milind Desai, MD, MBA, Vice Chair of Education for Cleveland Clinic’s Heart, Vascular & Thoracic Institute:

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/81e2f886-ca0a-464f-bc9f-e0c676406475/coronary-CT-angiography-inset)
Two applications of coronary CTA at Cleveland Clinic. Left image is a 3D rendering showing stenosis (arrow) of the proximal left anterior descending artery (LAD). Right image was taken in a separate patient after a bypass operation. It shows a patent left internal thoracic artery (LITA) with clips on its branches (bright white) anastomosed to the LAD beyond its diseased and calcified segments (also bright white).
He adds that newer techniques like CT fractional flow reserve (CT-FFR) use coronary CTA-derived data to simulate blood flow through the coronary arteries and calculate the FFR to assess the functional significance of a moderate coronary lesion. “CT-FFR can potentially be useful in determining, for example, whether a 50% to 70% stenosis on CT is flow-limiting or nonobstructive,” Dr. Desai explains. “This helps guide decisions related to revascularization.”
Advertisement

Resourceful approaches to the care of patients with microvascular disease and elevated Lp(a)

Cleveland Clinic’s new dedicated program offers nuanced care for a newly recognized cardiovascular risk factor

Structured interventions enhance sleep, safety and caregiver resiliency in high-acuity units

A scannable recap of our latest data in these clinical areas

Lutheran Hospital team brings emerging treatments to community setting

In the wake of NOTION-3 findings, a strong argument for physician judgment remains

The case for a thoughtful approach to CTO and minimally invasive options for CABG
Support for a TAVR-first approach in patients with concurrent valve and coronary disease