Locations:

Multidisciplinary focus on an often underdiagnosed and ineffectively treated pulmonary disease

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c946fda3-ae85-40ba-9b7c-1899a12c3590/senior-coughing)
Patient coughing
The Pulmonary Department at Cleveland Clinic has launched a new program devoted to researching and treating diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH). Discovered in 1992, DIPNECH is challenging to manage; with non-specific symptoms such as a dry cough and shortness of breath, it can be easily misdiagnosed as asthma or chronic obstructive pulmonary disease (COPD).1,2
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Treatment options have limited efficacy and lack a strong evidence base. DIPNECH is still labeled as an uncommon disease, likely because it can be difficult to diagnose and is often overlooked by clinicians to explain symptoms (chronic refractory cough with small nodules).
The DIPNECH clinic will include a multidisciplinary team led by pulmonologists with an interest in DIPNECH who will collaborate with thoracic pathologists, radiologists, surgeons and oncologists.
“We believe that there is an opportunity to better manage this condition, both in diagnosis and treatment. We know there are patients who are overlooked and could benefit from treatment,” says Uddalak Majumdar, MD, a pulmonologist at Cleveland Clinic who organized the program with Peter Mazzone, MD, MPH, Director of the Lung Cancer Program for the Integrated Hospital-Care Institute.
The World Health Organization (WHO) defines DIPNECH as a multifocal hyperplasia of pulmonary neuroendocrine cells often organized into tumorlets, which have the potential to develop into carcinoid tumors.3 Interestingly, DIPNECH cells express somatostatin receptors (SSTRs), which are a target for treatment (see treatment section below).
DIPNECH most often presents in women with a median age of 65 (more than 90%) who have never smoked. DIPNECH’s symptoms can sometimes be severe, like refractory cough which can be debilitating. Neuroendocrine cell hyperplasia can also often be seen secondary to other causes, and that also leads to complexities in diagnostic evaluation.
Advertisement
DIPNECH still lacks a universally accepted set of pragmatic diagnostic criteria;1 however, these clinical cues support a DIPNECH diagnosis: middle-aged female, chronic cough, spirometric obstruction, multiple small nodules, air-trapping and mosaicism.
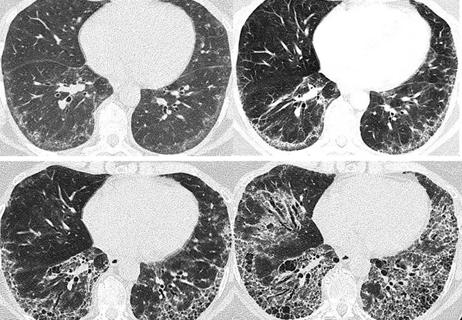
Laboratory testing is usually not useful to diagnose DIPNECH but can help rule out other conditions such as asthma. Chest x-ray cannot detect DIPNECH’s small nodules; CT scanning is the imaging modality of choice. Nodules are essential to diagnosis; multiple, non-calcified solid small nodules with sharp borders are visible on a CT scan.
For years, the only way to definitively diagnose DIPNECH was by surgical lung biopsy, which can often be challenging.4 A multidisciplinary assessment has been shown to improve accuracy in diagnosing DIPNECH without requiring an invasive procedure.5 “With the help of advanced imaging and multidisciplinary discussion, we can assess patients with chronic cough more comprehensively without resorting to invasive procedures like biopsies,” says Dr. Majumdar. Apart from DIPNECH, an idiopathic condition, clinicians also need to be aware of secondary neuroendocrine hyperplasia, in which neuroendocrine cells may be seen on a biopsy but are not the primary etiology of disease or symptoms.
Before an accurate diagnosis, DIPNECH patients often undergo years of ineffective therapies targeting better known obstructive lung diseases.6 Symptoms of bronchoconstriction, such as cough and wheezing, can be managed with inhalers containing beta-agonist-bronchodilators and inhaled corticosteroids.
Advertisement
If there is no response within six weeks, patients can be treated with somatostatin analogs (SSAs) which can improve symptoms and potentially restrict nodule growth. They can be managed at the DIPNECH clinic or another facility with this specialized expertise and patients can be trained on using injections at home. “In about half of patients, SSAs are effective. For those patients, going from constant coughing to not coughing is life-altering,” says Dr. Majumdar.
DIPNECH rarely leads to respiratory failure or death. Progression to overt carcinoid tumors may occur in some patients. “Tumors are part of the disease spectrum and may need to be removed but timing of surgery is not always clear given the indolent nature of the tumors,” says Dr. Majumdar.
Patients should be monitored; in some cases, lifelong surveillance is needed. DIPNECH patients have a 10-year survival rate of more than 70%.1
The DIPNECH program is developing a systematic approach to managing the disease. There is a published care path to guide general pulmonary clinicians to manage patients in the initial stages – getting CT scans with expiratory images, PFTs, starting inhaler therapy. If symptoms are still not controlled, patients can be evaluated at the DIPNECH clinic. Patients’ details are discussed at multidisciplinary meetings; in challenging cases, a consensus of two clinicians is required for a DIPNECH diagnosis.
The initial goals of the DIPNECH program are to educate clinicians about the disease, offer more effective treatment options like somatostatin analogs and help with deciding on surgical options. As the program progresses, the patient population will be studied and data analyzed. “We will collaborate with other centers to develop publications and conduct trials for novel medications,” says Dr. Majumdar.
Advertisement
To refer patients who present with DIPNECH symptoms, contact Dr. Uddalak Majumdar (majumdu@ccf.org, 216-445-1701 option 2) or Brenda Bolenski, coordinator (bolensb@ccf.org, 216-445-0647).
References
Advertisement
Advertisement

Overexposure to the common alloy can lead to an autoimmune response called sensitization

A look into recent developments in the diagnosis of LAM and its clinical presentation

A review of treatment options for patients who may not qualify for surgery

Rising rates in young miners illustrate the need for consistent prevention messaging from employers and clinicians

Management and diagnostic insights from an infectious disease specialist and a pulmonary specialist

Treatments can be effective, but timely diagnosis is key

A Cleveland Clinic pulmonologist highlights several factors to be aware of when treating patients
Patient experience improves with a multidisciplinary approach