Locations:

Retrospective findings from an executive health program spur interest in broader studies
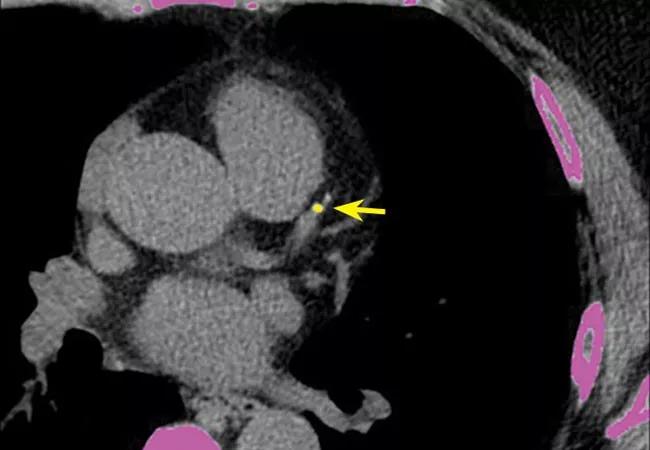
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/517d1e34-b871-4f0d-a52b-ab4005b15964/23-HVI-3606662_calcium-scoring_650x450_jpg)
23-HVI-3606662_calcium-scoring_650x450
A Cleveland Clinic study presented at the American College of Cardiology’s 2023 Scientific Session found a strong association between coronary artery calcium (CAC) score and the presence of carotid artery plaque but not of significant carotid stenosis.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Plaque buildup was ubiquitous, but on the bright side, severe carotid plaque was not,” says cardiologist and principal investigator Milind Desai, MD, MBA, Director of Clinical Operations in Cleveland Clinic’s Department of Cardiovascular Medicine.
The study involved 2,801 asymptomatic individuals who underwent screening carotid duplex ultrasound and coronary artery calcium (CAC) scoring as part of an executive health workup at Cleveland Clinic between March 2016 and October 2021. The cohort was relatively young (median age, 59 years) and predominantly white (87%) and male (71%).
Higher amounts of plaque in the coronary arteries correlated with higher amounts in the carotid arteries. “This was no surprise, since we know atherosclerosis begets atherosclerosis,” says Dr. Desai. “Yet despite a fair amount of coronary plaque, the number of individuals with severe carotid stenosis was very, very low. This was a bigger surprise.”
Nearly half (49%) of the cohort had no carotid plaque, whereas 27% had bilateral carotid plaque, 11% had only right-sided plaque and 13% had only left-sided plaque.
The presence of carotid plaque rose in tandem with Multi-Ethnic Study of Atherosclerosis (MESA) CAC risk scores.
No individual was found to have carotid stenosis of 70% or more. Only 19 (0.7%) had carotid stenosis between 50% and 69%, and 1419 (50%) had stenosis of 50% or less in either carotid artery.
“We don’t know why there was plaque buildup without significant narrowing,” says Dr. Desai. “The Glagov phenomenon may be at play here. This causes the arteries to enlarge to accommodate plaque without compromising blood flow through the lumen. Alternatively, it’s possible that different mechanisms are driving plaque buildup in the two locations.”
Advertisement
“Coronary artery disease is more prevalent than peripheral arterial or cerebrovascular disease, so these findings are not particularly surprising,” adds study co-author Leslie Cho, MD, Co-Section Head of Preventive Cardiology at Cleveland Clinic.
Because the study was conducted in asymptomatic individuals, these findings underscore the importance of continued vigilance for atherosclerosis, starting at a young age and continuing over time, Dr. Desai notes.
“Equally important,” he adds, “when atherosclerosis is identified, it must be treated aggressively with statins, blood pressure control, weight control and other proven methods of risk-factor modification.”
Dr. Cho concurs. “These findings speak to the importance of controlling risk factors, since atherosclerosis in one bed frequently begets atherosclerosis in another territory,” she says.
One common benefit of these screening tests is increased compliance with preventive measures. “Asymptomatic patients often think there’s nothing wrong with them and they are invincible,” Dr. Desai observes. “When we show them the scans, their refusal to take statins or make lifestyle changes often will suddenly melt away.”
Cleveland Clinic cardiologists have collaborated with executive health providers to conduct CAC scoring for several years. Initially, the program was so well received that CAC scoring was made available to any Cleveland Clinic patient requesting it. As a result, the database contains CAC scores on thousands of individuals and carotid duplex data on nearly as many.
Advertisement
This study was the first to explore whether there is a potential connection between the two areas of plaque buildup. Additional analyses are forthcoming. “We also need to do serial follow-ups to see whether these tests add incremental prognostic value,” Dr. Desai says.
He notes that the current study was limited by its predominant focus on white men who referred themselves for screening physicals. “We need to use the data we have on a broader population to look for whether plaque behaves differently in men or women of different ethnicities,” he concludes.
Advertisement
Advertisement

Maintain a high index of clinical suspicion and consider the underlying etiology

5 biggest changes according to Cleveland Clinic experts
While procedural success rates lag overall, they shine for retrograde crossing
Lower success rates, more hospital MACE seen with poor-quality distal targets

Important additions to a novel surgical technique
Growing awareness of impact leads to proliferation of procedures

How to talk about lifetime risk, treatment goals, Lp(a) testing, statin skepticism and more

Post hoc analysis of SURPASS-CVOT trial has implications for future cardiovascular outcome trials