Locations:

Disagreement on both sides of Atlantic about classic RCVS case
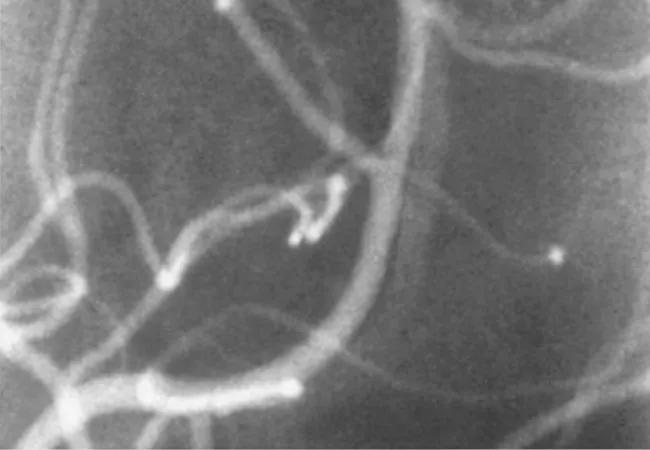
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ce776106-c038-424f-a506-0796e05a2f34/16-RHE-871-Calabrese-Hero-Image-650x450pxl_jpg)
16-RHE-871-Calabrese-Hero-Image-650x450pxl
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 63-year-old generally healthy woman with a history of migraine was vacationing in Tuscany with her husband in July 2013. She dived into a cold swimming pool for her customary early morning swim. After swimming three laps, she experienced the worst headache of her life, “which came on like a rocket.” She did not lose consciousness, but felt some confusion. She decided to sleep, and awakened after a few hours with continued headache and confusion, in addition to nausea and vomiting. After contacting her general practitioner in their home of New York City, her husband transported the woman to an emergency room in Siena, Italy.
A CT scan revealed a small subarachnoid hemorrhage, and the woman was admitted to the intensive care unit. The headache subsided but returned 12 hours later. An angiogram and MRI demonstrated multiple areas of stenosis and beading, and again the headache subsided. Three days later, still hospitalized, the headache flared again after a “cold” bath. Another CT scan showed additional bleeding. At this point, she was air evacuated to New York City.
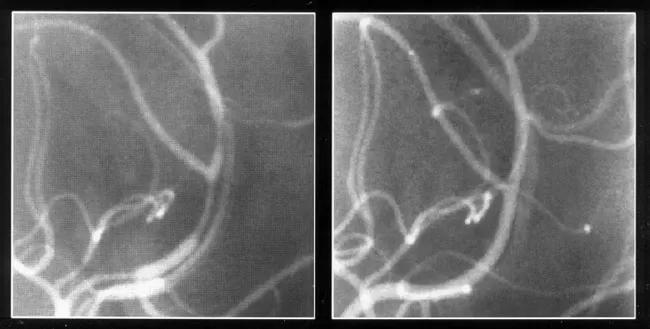
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1dd6790d-5074-4e5d-b887-453e4bd903d4/16-RHE-871-Calabrese-Inset-Image-650pxl-width_jpg)
Cerebral angiograms showing areas of multiple vascular stenosis in a case of RCVS (left), and clearing of anomalies six weeks later (right).
In the city, neurologists ruled out aneurysm and recognized vascular irregularities indicative of spasms or vasculitis of the central nervous system. She was treated with a front line immunosuppressive regimen for vasculitis. Her headaches subsided, but she continued to feel unwell over the next several weeks. Her team referred her to a rheumatologist in New York, who astutely recognized that her symptoms and history, coupled with her 10-year use of selective serotonin reuptake inhibitors (SSRIs), suggested a different diagnosis: reversible cerebral vasoconstriction syndrome (RCVS).
Advertisement
This rheumatologist called me, and I agreed to see the patient immediately. She and her husband drove to Cleveland.
Based on the totality of her presentation, we confirmed a diagnosis of RCVS, suggested halting her immunotherapy and explained that her case was classical in every regard, including her relapse over the first three weeks. We informed her that cold exposure can trigger RCVS and that our studies have demonstrated that RCVS is unlikely to recur after the initial episode. We suggested that she stop the SSRI as well, practice relaxation techniques (mindful meditation and yoga), change her diet and avoid certain other medications.
As the patient noted in her 2014 letter to Cleveland Clinic: “I have known since last autumn that I was not suffering from what had been diagnosed as a debilitating and likely progressive case of vasculitis. Rather, I had experienced and was recovering from the much less lethal RCVS.” The relieved patient continues to do well three years later and follow-up MRI and ultrasounds have normalized.
RCVS is likely a disturbance in the cerebral vascular regulatory tone, though the precise mechanisms responsible for this derangement remain unknown. RCVS is associated with subarachnoid hemorrhage and less commonly ischemic or hemorrhagic stroke in approximately 30 percent of patients. Posterior reversible encephalopathy syndrome has a similar presentation, and is found in 25 percent of RCVS patients.
An amazing array of instantaneous, seemingly irrelevant precipitants can induce RCVS. In this case it was exposure to cold, but we have also seen triggers of emotional stress, such as public speaking anxiety; sexual activity; showering; having a bowel movement; coughing or intense emotion. I treated an actress doing a death scene in Shakespeare who collapsed to the stage with the characteristic thunderclap headache.
Advertisement
Those who are well-versed in identifying RCVS can practically make the diagnosis over the phone. For those who are not, it is a profound diagnostic conundrum.
We emphasize the following five criteria that must be fulfilled for a definitive diagnosis of RCVS:
We first described these criteria in our 2007 seminal article on RCVS in the Annals of Internal Medicine. RCVS is a disease our group has defined and investigated over the past 25 years; we have become a clinical leader in this disorder and see several patients a month.
Five out of six patients with RCVS are women, suggesting hormonal factors. Prescription drugs and drugs of abuse are also associated with RCVS. SSRIs and marijuana are very common precipitants. Sympathomimetic vasoconstrictors, decongestants, cocaine, amphetamines and herbal preparations also have been implicated.
Frequently patients are not forthcoming about precipitating factors – such as sexual activity or medication use. We ask patients to bring all of their medications and supplements to an appointment.
Under the direction of my colleague, Rula Hajj-Ali, MD, we have developed a robust research approach to this disorder and the R.J. Fasenmyer Center for Clinical Immunology biobank collects blood, DNA, RNA and cerebrospinal fluid samples from RCVS patients. We hope to identify biomarkers that will help outline the pathogenesis of RCVS, improve diagnosis, identify therapeutic targets and develop better treatments and preventive strategies.
Advertisement
That this patient’s classical presentation was not clinically appreciated on both sides of the Atlantic illustrates the need for more awareness across the profession, especially since patients with RCVS often present to other specialties, including neurology, gynecology and primary care. I am hopeful that knowledge of the RCVS diagnosis will continue to grow among physicians of all specialties. This will help reduce misdiagnosis and avoid unnecessary immunosuppressive therapy for hundreds of people.
Dr. Calabrese is Director of the R.J. Fasenmyer Center for Clinical Immunology in Cleveland Clinic’s Department of Rheumatic and Immunologic Diseases.
Advertisement
Advertisement

Researching the biological basis for why treatment is or is not effective

Scribing system helps create more face-to-face interactions

A conversation with Leonard Calabrese, DO

The case for continued vigilance, counseling and antivirals

High fevers, diffuse rashes pointed to an unexpected diagnosis

No-cost learning and CME credit are part of this webcast series

Summit broadens understanding of new therapies and disease management

Program empowers users with PsA to take charge of their mental well being