Is the gut microbiome the body’s largest endocrine organ?
There’s been another shake-up in our understanding of the causes of cardiovascular disease. Cholesterol is still king. But it now shares explanatory power with a swarm of bacteria resident in the digestive tract. The first studies of these bacteria (reviewed here) found direct links between the chemical product of their metabolism and the vascular events leading to heart attack. Now studies are linking these bacteria to heart failure and even chronic kidney disease.
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“The concept that gut flora contribute not only to atherosclerosis, but also to heart failure and chronic kidney disease, opens up exciting new nutritional and interventional prospects,” says Stanley Hazen, MD, PhD, Chair of Cellular and Molecular Medicine and Section Head of Preventive Cardiology and Rehabilitation at Cleveland Clinic.
Dr. Hazen served as principal author of key clinical studies published in the spring of 2013 — one in New England Journal of Medicine and another in Nature Medicine. These studies showed how certain bacteria found primarily in the intestines turn choline — a byproduct of lecithin, found in meat and eggs — into trimethylamine (TMA), which is absorbed into the bloodstream and metabolized by the liver. There, it is transformed into the substance that appears to be a key player in a number of disease processes: TMAO. These studies also showed a clear link between higher TMAO levels and elevated three-year risk of heart attack, stroke and death.
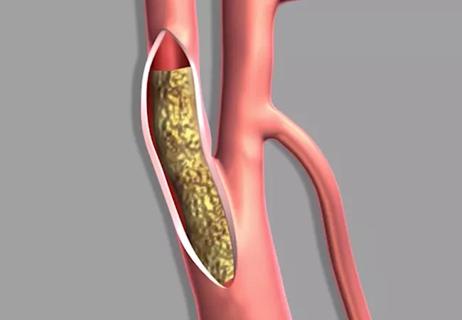
Gut bacteria may affect the progress of cardiovascular disease by influencing appetite, fat creation and insulin sensitivity. But the key process involves how the host digests two key nutrients, choline and L-carnitine. Choline is abundant in animal cell membranes, egg yolk and high-fat dairy products; L-carnitine is found mostly in red meat. They also are marketed as nutritional supplements, with L-carnitine being a frequent ingredient in energy drinks.
When dietary choline and L-carnitine come in contact with certain bacteria in the intestine, they are metabolized into TMA, which makes its way to the liver through the portal circulation, where an enzyme converts it to TMAO (trimethylamine-N-oxide). TMAO ends up in the bloodstream, where it participates in changes in whole-body cholesterol metabolism, vascular inflammation and formation of unstable plaques in the arterial walls.
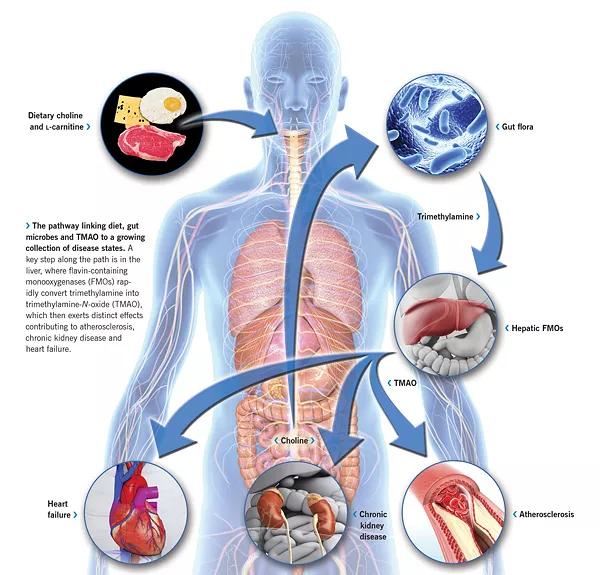
Schematic of the pathway linking diet, gut microbes and TMAO to a growing collection of disease states. A key step along the path is in the liver, where flavin-containing monooxygenases (FMOs) rapidly convert trimethylamine into trimethylamine-N-oxide (TMAO), which then exerts distinct effects contributing to atherosclerosis, chronic kidney disease and heart failure.
A new study from the Hazen lab, published in Cell Metabolism, has revealed an additional metabolite of L-carnitine that may be involved in atherosclerosis development. Known as γ-butyrobetaine, it is a newly discovered intermediate that is formed in large amounts by gut microbes and ultimately gets turned into TMAO. After being produced in the proximal gut by one set of microbes, the γ-butyrobetaine is converted into TMA lower in the gut by a distinct set of microbes. These studies are of interest, Dr. Hazen notes, because they identify a new set of microbial targets to help curb the TMAO generation in response to dietary L-carnitine.
Dr. Hazen and his team have developed a test that can help assess cardiac risk by measuring plasma TMAO. It has already been used in several clinical studies of well over 5,000 subjects collectively, which have shown it to predict increased cardiovascular risk. Although the test is currently available only for research purposes, several diagnostics companies are expressing interest in making it more widely available, perhaps as early as this year.
“TMAO is readily measured using mass spectrometry, which is a widely used platform for diagnostic testing available at larger reference labs,” explains Dr. Hazen. “We expect that testing for TMAO may one day help us individualize dietary recommendations and also facilitate monitoring of gut microbe-targeted therapies.”
Chronic kidney disease is increasing in prevalence and represents a major healthcare cost burden. It’s also strongly linked to cardiovascular disease risk.
“We’ve found that the TMAO pathway seems to be mechanistically linked not only to atherosclerosis but also to the development of chronic kidney disease, based on animal model data and some human studies,” says Dr. Hazen.
In a new paper in Circulation Research, Dr. Hazen, together with W.H. Wilson Tang, MD, and other Cleveland Clinic colleagues, showed in animal models that chronic consumption of dietary choline (the precursor for forming TMAO) or TMAO itself appears to directly contribute to progressive renal fibrosis and dysfunction. They also examined 3,166 subjects with normal kidneys, plus another 521 subjects with chronic kidney disease, and followed their medical history over five years. They confirmed that high blood levels of TMAO at baseline were associated with chronic kidney disease and also with poorer outcomes and higher five-year mortality among subjects with and without kidney disease. TMAO was found to predict worse outcome particularly among those with less than normal kidney function.
“People with chronic kidney disease and end-stage renal disease tend to die of heart disease,” says Dr. Hazen. “Even when their kidney function is replaced, they still die of heart disease. In fact, traditional risk factors don’t adequately account for the heightened cardiovascular risks observed in subjects with kidney disease. Recent animal model studies and human clinical studies collectively indicate that elevated TMAO may contribute to renal functional impairment, which further raises TMAO levels, and is associated with progressively worse cardiovascular risks.”
New studies by Dr. Hazen, Dr. Tang and colleagues also link TMAO to both systolic and diastolic heart failure. One paper, published in the Journal of the American College of Cardiology, examined the relationship between gut flora-dependent TMAO and all-cause mortality in 720 patients with stable heart failure over five years. It found that these patients had elevated TMAO — and that the higher the TMAO, the higher the long-term mortality risk, independent of traditional risk factors, renal function and markers of heart strain like B-type natriuretic peptide (BNP). In patients with both high TMAO and high BNP, the five-year mortality rate was greater than 50 percent.
The findings imply that testing for TMAO may help identify which patients are at higher risk from heart failure. And while this concept is not yet tested, they also suggest that new dietary strategies to prevent TMAO elevation may be beneficial for patients with heart failure or kidney disease.
Dr. Hazen believes we are only at the beginning of our understanding of the complex relationships among our gut bacteria and our organ systems. Among the goals of his lab is to establish the mechanisms by which TMAO promotes atherosclerotic disease.
“Data show that TMAO and this pathway are centrally involved in cholesterol and sterol metabolism, both by impacting how cholesterol is taken up by cells in the artery wall and by inhibiting removal of cholesterol from the artery wall, reducing what is called reverse cholesterol transport,” Dr. Hazen notes. “The net effect is buildup of cholesterol in cells of the artery wall. But it’s clear that this is not the complete story: TMAO seems to foster changes in cellular metabolism that make a person more susceptible to cardiovascular events such as heart attack, stroke and even death. We and others have many studies on this subject in the pipeline.”
Dr. Hazen is particularly excited about a study his group just published in the Journal of Biological Chemistry. “It demonstrates for the first time that we can fulfill Koch’s postulate of causation, showing that microbial transplantation can transfer susceptibility for development of atherosclerosis in an animal model,” he explains. Studies such as these firmly establish a mechanistic link between gut microbes and cardiovascular disease.
Dr. Hazen adds that many future research needs relate to identifying specific metabolites that are relevant to disease and the gut microbial enzyme systems involved in generating these compounds — along with their host receptor systems.
“Our gut bacteria serve as a filter of our largest environmental exposure — the food we eat,” he says. “It’s reasonable to think of the intestinal microbiome as our largest endocrine organ. Just consider that the gut microbiome makes biologically active compounds that circulate in the body and impact end-organ physiology just like hormones do. But it’s a flexible endocrine organ, and what it’s fed over time can influence what it becomes. Once we work out the chemical language of this organ, we can develop drugs to manipulate it and reduce the risk of cardiovascular disease, heart failure, kidney disease and possibly a host of other conditions.”
Dr. Hazen has studies underway to “drug” the microbiome with medications and perhaps with probiotics or other substances that may be able to suppress specific bacteria to safely inhibit their endocrine effect on distant organs.
“This field is moving fast,” he says. “One study builds on another. And many groups are jumping into the field. There is still much to be told — and much, much more to learn.”

Surprise findings argue for caution about testosterone use in men at risk for fracture

Findings support emphasis on markers of frailty related to, but not dependent on, age
![GettyImages-1252287413 [Converted]](https://assets.clevelandclinic.org/transform/StoryPanel/350804b2-f1e4-4d97-a277-9629cf45af3e/23-HVI-4120348_redlining_650x450_jpg?w=3840&q=75)
Large database study reveals lingering health consequences of decades-old discrimination
Additional analyses of the two trials presented at 2023 ESC Congress
Prospective SPIRIT-HCM trial demonstrates broad gains over 12-month follow-up

An ACC committee issues recommendations to accelerate sluggish progress
Review of our recent experience shows it’s still a safe option
Machine learning may improve risk prediction and guide therapy