Locations:

A rare fibroproliferative disorder
By Soumya Chatterjee, MD, MS, FRCP, and Steven D Billings, MD
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A woman aged 66 years, with a history of nodal osteoarthritis, presented with cutaneous nodules on her fingers and flexion contractures. The patient was no longer able to make a fist or straighten her fingers completely (figure, A). Her second to fifth metacarpophalangeal, proximal interphalangeal and distal interphalangeal joints were swollen and tender. There were several firm, red, raised, tender cutaneous nodules (figure, A, inset). The patient also had a firm, non-tender swelling over the extensor aspect of the right forearm (figure, B). There were no psoriatic skin or nail changes.
Laboratory studies yielded normal results (complete blood count, comprehensive metabolic panel, inflammatory markers, serum uric acid, rheumatoid factor, cyclic citrullinated peptide antibody, antinuclear antibody and antibodies to extractable nuclear antigens).
Radiographs of the patient’s hands showed soft tissue swelling, an erosion at the left ulnar styloid, and multiple intra-articular erosions at the proximal interphalangeal and distal interphalangeal joints bilaterally (figure, C). Radiographs of the patient’s feet also showed multiple scattered peri-articular and intra-articular erosions at the proximal interphalangeal and distal interphalangeal joints (figure, D).
A biopsy from one of the cutaneous nodules located on the left second finger showed predominantly acellular dense dermal fibrosis with a loss of elastic fibers and the presence of myofibroblasts (figure, E–G).
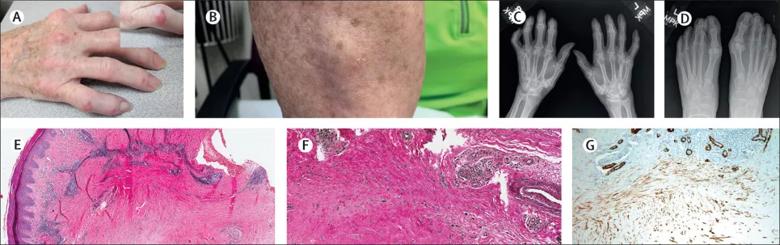
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/82f08ee1-221d-40fb-b818-eb13712c16ec/fibroblastic-rheumatism_jpg)
Erosive arthritis and joint contractures with nodular skin lesions. (A) Swollen metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints of second to fifth fingers associated with cutaneous nodules (inset) and flexion contractures. (B) Swelling over the extensor aspect of the right forearm. (C) Hand radiographs showing soft tissue swelling, an erosion at the left ulnar styloid, and multiple intra-articular erosions at the proximal interphalangeal and distal interphalangeal joints bilaterally. (D) Foot radiographs showing multiple scattered peri-articular and intra-articular erosions at proximal interphalangeal and distal interphalangeal joints. (E) Haematoxylin and eosin-stained biopsy of a cutaneous nodule showing predominantly acellular dense fibrosis in the deep dermis, with a superficial perivascular lymphocytic infiltrate (magnification × 40). (F) The elastic stain (Verhoeff-Van Gieson stain) indicated a loss of elastic fibers in the area of dermal fibrosis (magnification × 100). Elastic fibers stain black, and they are mostly absent in the region of fibrosis. There are remnants of normal elastic fibers in the upper left-hand corner of the image and around the larger blood vessel. (G) Immunohistochemical staining for smooth muscle actin highlights the myofibroblasts within the dense region of fibrosis.
Advertisement
The clinical and pathological findings of the patient were consistent with the diagnosis of fibroblastic rheumatism.
The patient responded to weekly methotrexate (10 mg). The skin nodules stopped growing, with no new lesions. The patient’s joint pain improved, and her flexion contractures stabilized.
Fibroblastic rheumatism is a rare fibroproliferative disorder, characterized by the sudden onset of symmetrical inflammatory polyarthritis associated with multiple, firm, tender, flesh-colored to purplish cutaneous nodules (2–20 mm in size), typically on extensor surfaces of metacarpophalangeal and interphalangeal joints, and also over other peri-articular sites (e.g., elbows, knees, ankle and feet). Permanent flexion contractures of the fingers can develop rapidly. Laboratory investigations usually yield normal results. Radiography shows soft tissue swelling, which can progress to an erosive arthropathy. Histological findings vary from scar-like, fibromatosis-like, to relatively acellular (i.e., morphea-like or nuchal fibroma-like) fibrosis.
Diagnosis of fibroblastic rheumatism is based on characteristic clinical findings in combination with histopathological findings. The differential diagnosis of multiple cutaneous nodules and arthropathy includes rheumatoid arthritis, gout, calcinosis, tendon xanthomas, multicentric reticulohistiocytosis and nodular scleroderma. Based on scarce available data, glucocorticoids or methotrexate, or both, are the most effective disease-modifying drugs.
Advertisement
Note: Republished with permission from Lancet Rheumatology. Originally published as: Chatterjee S, Billings SD. Hand contractures and skin nodules in a 66-year-old woman. Lancet Rheumatol. 2020; 2:e646.
Advertisement
Advertisement

Family history may eclipse sun exposure in some cases

Consider secondary syphilis in the differential of annular lesions

Persistent rectal pain leads to diffuse pustules

Two cases — both tremendously different in their level of complexity — illustrate the core principles of nasal reconstruction
Stress and immunosuppression can trigger reactivation of latent virus

Low-dose, monitored prescription therapy demonstrates success

Antioxidants, barrier-enhancing agents can improve thinning hair
