Locations:

Success lies in a systematic, data-driven, communication-oriented approach
The pressures in healthcare today are nearly universal: Accommodate higher volumes. Improve quality and outcomes. Optimize patient experience. And do all of this while keeping costs to a minimum without compromising patient care.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Helping other hospitals and health systems balance these seemingly competing challenges is a primary goal of Cleveland Clinic’s Miller Family Heart & Vascular Institute Affiliate Program. This is the objective of the program’s Continuous Improvement Service (i.e., CI team), which provides advisory services to healthcare organizations across the U.S. Some of these organizations partner with Cleveland Clinic as affiliates for cardiovascular care. The Affiliate Program team also does assessments of specific clinical or operational challenges in affiliates’ cardiovascular programs.
The Affiliate Program recognizes that healthcare value is driven through four key areas: quality and reporting, clinical care delivery, cost containment and programmatic growth. The program’s CI team focuses on cost containment and programmatic growth in recognition that both can stem from efficiency improvement. Specifically, more-efficient operations tend to save costs in equipment, staff time, etc., while potentially freeing up facilities and staff to care for more patients and grow program volumes.
The CI team’s approach is modeled on insights gained through experience with projects completed in Cleveland Clinic’s internationally recognized cardiovascular program. An example of such a project is a catheterization lab process improvement initiative whose results are summarized in the graphic below.
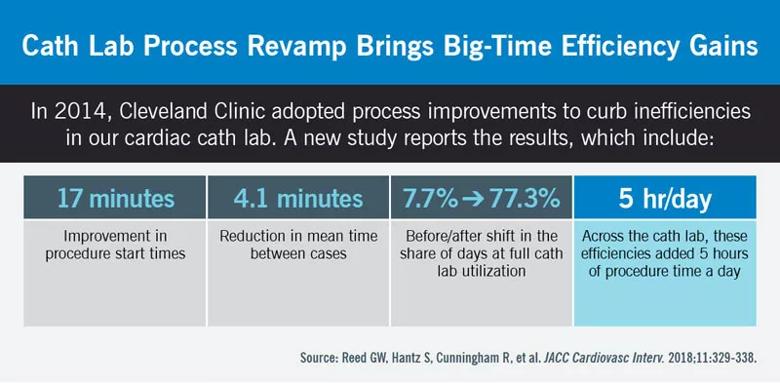
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/be9917b4-7290-4a21-a5c4-7ac9ecb98bda/18-HRT-4698-Inset-1_jpg)
The CI assessment focuses on identifying opportunities for efficiency improvement, cost reduction and program growth throughout the affiliate hospital’s cardiovascular service line. The CI team completes this assessment by following a systematic data-driven approach as illustrated below:
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4d82595f-5561-4e0c-8bdf-8f7f4187474f/18-HRT-4698-Inset-2_jpg)
As a part of the data analysis phase, the CI team completes a thorough operational analysis. Following are some of the operational metrics analyzed for cath/electrophysiology labs and operating rooms:
These metrics are benchmarked to Cleveland Clinic metrics, just as national registries (e.g., the Society of Thoracic Surgeons database) serve as benchmarks for quality metrics and best-practice implementation efforts.
This approach to data submission and analysis yields many benefits, including:
Industry-proven CI methodologies, such as Lean and Six Sigma, are used throughout the process. The CI team works closely with Cleveland Clinic Heart & Vascular Institute physicians and clinical consultants for each area/subspecialty to provide well-rounded recommendations that include both clinical and operational perspectives.
Based on the list of recommendations, the CI team works with the affiliate hospital’s administrative, physician and clinical teams to prioritize areas of focus. They then determine a project implementation plan for these areas using the Plan-Do-Check-Act approach to drive improvements and sustain gains.
Advertisement
This type of CI assessment was completed at more than 20 hospitals across the country, and the team identified several opportunities for efficiency improvement and cost reduction. Examples include:
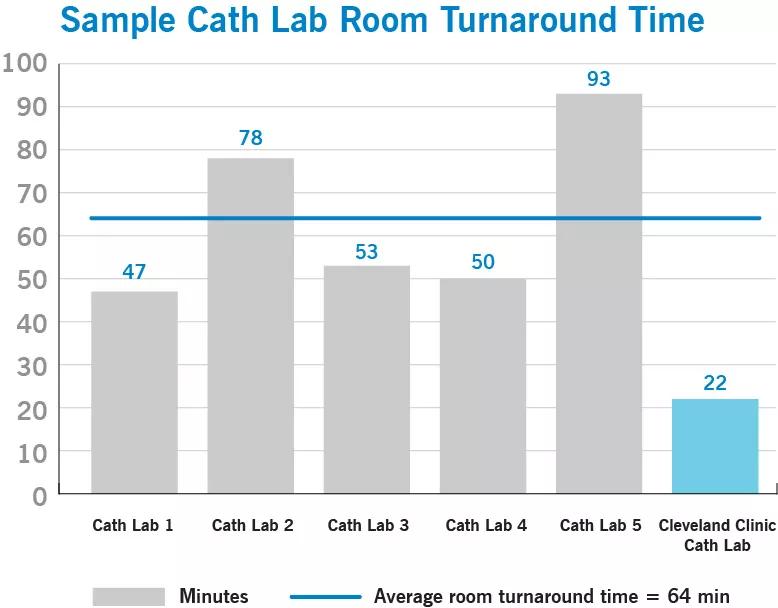
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7834885f-21e2-4c62-be9a-0f65ebe12d1b/18-HRT-4698-Inset-3_jpg)
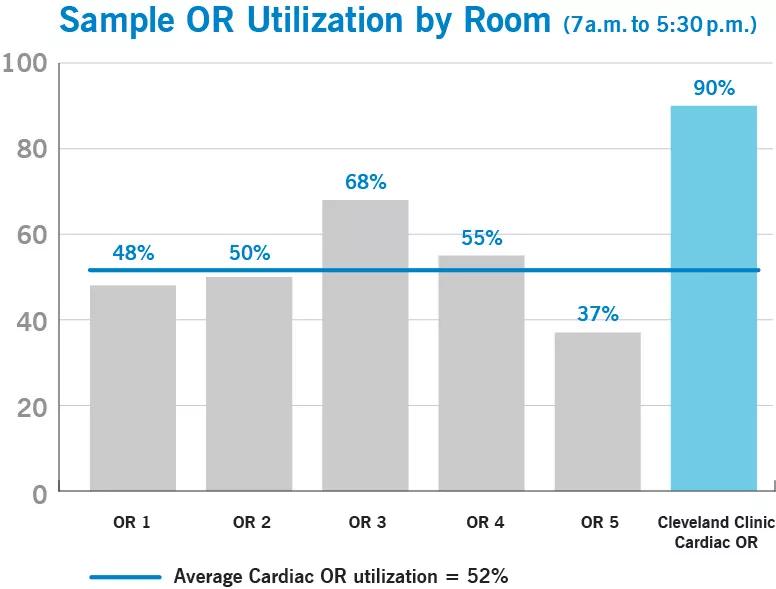
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e10684bd-9da3-4a58-8011-6c0b12629360/18-HRT-4698-Inset-4_jpg)
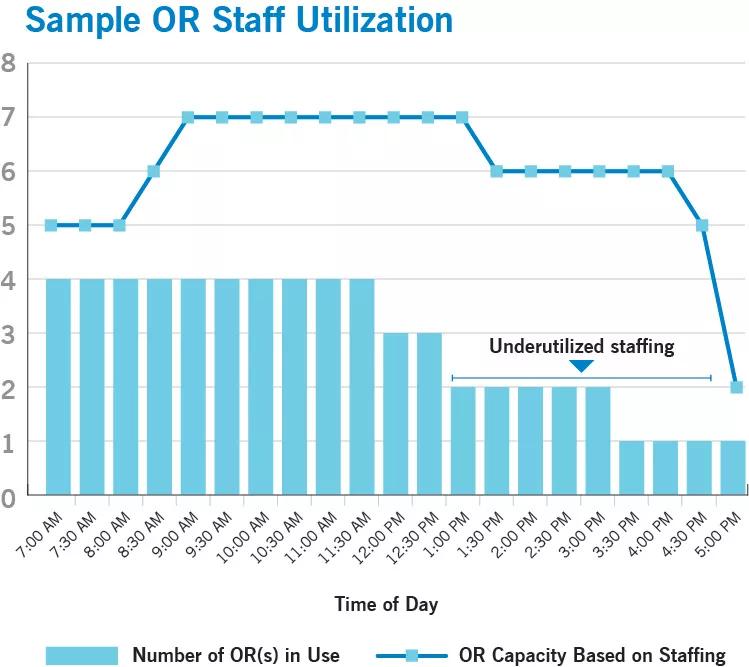
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7ccb7e3d-3009-4309-8f93-5dc4810d3616/18-HRT-4698-Inset-5_jpg)
The thorough and systematic process outlined above provides insight into affiliate hospitals’ operations down to a highly detailed level. It also facilitates communication of key operational issues and opportunities to their clinical teams and administrative leadership while aligning CI efforts with strategic enterprise initiatives. Identifying specific areas to focus on enables feasible plans to be put in place for steady progress toward program goals.
Advertisement
These services from the CI team are included in the scope of offerings from Cleveland Clinic’s Heart & Vascular Institute Affiliate Program and are central to efforts to drive down cost while improving quality, patient flow and overall service line excellence.
For more information, contact Murali Dodla (dodlam@ccf.org) or Christina Seekely (seekelc@ccf.org).
Advertisement
Advertisement

New framework better distinguishes stable from critically ill patients

CMR-CLIP outperforms general AI tools; may one day expand patient access to CMR

Post hoc analysis of CLEAR Outcomes trial bolsters its case as a statin alternative

Large retrospective analysis may prompt prospective studies

How to talk about lifetime risk, treatment goals, Lp(a) testing, statin skepticism and more

A scannable recap of recent volumes and clinical metrics from Cleveland Clinic

Cleveland Clinic reports first U.S. series focused on use in this challenging setting

Large series confirms early and long-term survival advantages over partial pericardial resection