Locations:

How our HVTI Advisory Services team facilitated swift improvements for an allied health organization

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/cf968035-971e-4ff2-932b-66ed50fe24b8/1281256060)
older women being pushed in wheelchair in hospital
Consistent analysis of clinical operations and an ability to adapt plans of care to meet the needs of patients are critical to growth, efficiency improvement, wise resource allocation, cost containment and provision of safe and high-quality care. Healthcare organizations develop strategies and implement enhanced workflows to increase access to services, improve efficiencies and enhance patient experience.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
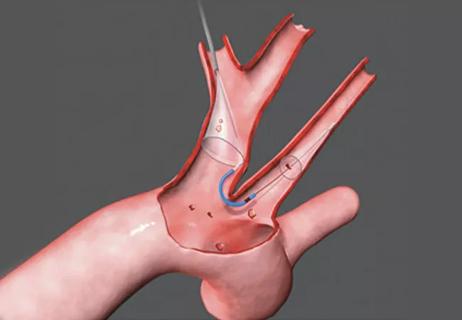
Transcatheter aortic valve replacement (TAVR) and other percutaneous valve procedures are increasing in prevalence, so optimizing workflows is important to cardiovascular service line success. Transitioning patients determined to be low risk for TAVR procedures to same-day discharge, rather than admission to an intensive care unit, is one strategy that offers several benefits for patients and organizations.
That is the experience of The Valley Hospital, which recently collaborated with the Advisory Services team of Cleveland Clinic’s Heart, Vascular & Thoracic Institute (HVTI) to drive improvements in the recovery and discharge of its patients undergoing TAVR. The Valley Hospital, which is part of Valley Health System serving northern New Jersey and southern New York, is a fully accredited, acute care, not-for-profit hospital that has had an alliance relationship with Cleveland Clinic’s HVTI since 2015.
Postprocedural care for TAVR patients can range from critical care admission to same-day discharge. The Valley Hospital recently assessed its processes for TAVR patient management and discharge and identified an opportunity for enhancement. Valley noted that 100% of TAVR patients were transferred to the cardiac surgery intensive care unit (CSICU) for recovery. This suggested there was an opportunity to develop a streamlined process to identify low-risk patients who would benefit from a fast-track recovery strategy. This change in patient throughput would also open bed capacity in the CSICU that could be used for acute patients requiring that level of care.
Advertisement
Valley sought to establish better-defined TAVR admission and discharge criteria, recognizing that appropriate, tailored postprocedural management of TAVR patients provides optimal patient experience without compromising patient outcomes or safety. The objectives were to align with industry best practice for TAVR recovery, increase the availability of the hospital’s critical care resources for the most acute care needs, enhance patient experience and reduce the economic burden of TAVR care.
To help achieve its objective, Valley enlisted the assistance of Cleveland Clinic’s HVTI Advisory Services team. The team conducted a rapid improvement event (RIE), also known as a Kaizen event, with members of Valley’s cath lab, same-day medicine and step-down unit teams, all of which are central to TAVR care and recovery.
Successful RIEs are driven by cross-functional teams to ensure buy-in. They are designed to rapidly yield measurable results by analyzing and improving a narrowly defined process where solutions have not yet been identified.
The RIE is part of the Lean Six Sigma process improvement approach, which tends to achieve the greatest success when used by individuals with expertise in utilizing Lean Six Sigma tools. The HVTI Advisory Services continuous improvement team brought that expertise to bear by helping the Valley multidisciplinary team assess TAVR processes and analyze recovery and discharge data. The teams could then determine the root cause of the issue, design experimental solutions, implement systems-based thinking, develop process efficiencies and outline standardized workflows.
Advertisement
Since the data showed 100% of TAVR patients were admitted to and recovered in the CSICU, and the team’s RIE process identified a need for new standardized workflows, criteria for patient transfer between units and indications for admission to a step-down unit needed to be developed. The group also recognized that it was imperative that these new workflows be effective in improving patient flow and optimizing care delivery.
The process led to defining a target state (Table), which was set in collaboration with Valley’s leadership and finance teams and guided by best practices for cath lab services and continuous improvement from Cleveland Clinic’s HVTI.
The Valley team and leaders, together with HVTI Advisory Services continuous improvement personnel, implemented the RIE methodology and visualized their processes for TAVR care. The multidisciplinary team identified 84 improvement opportunities in the recovery, admission and discharge processes. They were broadly categorized as follows: standard work, systems thinking, siloed teams, education and training, visual management, and patient flow. The team then proposed solutions and designed rapid experiments to meet its vision using Cleveland Clinic best practices and structured facilitation.
After developing written criteria and standardized workflows and applying the rapid experiments they had designed, the Valley team met most of its targets within 30 days of the RIE, and the changes enabled the team to realize a savings of $1,677 per TAVR patient and a cumulative $16,770 savings within 90 days (Table).
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/7d7cf526-7034-42d9-b6e7-e5f83d0aa031/table-on-progress-RIE-effort)
“Keys to success were the collaboration between the Cleveland Clinic and Valley teams and the engagement and backing of Valley executive leadership, which supported the RIE and committed the necessary time for the team to participate,” says Suma Thomas, MD, MBA, Vice Chair of HVTI Strategic Operations. She notes that this enabled a multidisciplinary team — which faced numerous deadlines and staffing challenges — to pause its day-to-day work to complete the RIE with 4.5-day attendance and full commitment.
Executive leaders trusted the process, nurtured a team spirit and instilled confidence in the Valley team members. Their support created an environment that allowed team members to take ownership of the initiative by designing their own solutions, which enhanced the team’s commitment to sustaining and achieving the RIE’s outcomes.
“The partnership and expertise of Cleveland Clinic’s continuous improvement team facilitated our advancement in the care of our TAVR patients while engaging our clinical and administrative teams,” says Derrick Lieb, DNP, MS-HCM, RN, NEA-BC, Assistant Vice President of The Valley Heart and Vascular Institute.
“Including frontline staff in the design and decision-making is key to sustaining changes,” adds Josh Gregoire, MS, MPH, RN, NEA-BC, Assistant Vice President of Quality/Performance Improvement and Clinical Operations. “It’s exciting to observe staff as they realize the important role they play in questioning and reinforcing processes.”
For information on affiliation or alliance opportunities with Cleveland Clinic’s Heart, Vascular & Thoracic Institute, email Amanda Lesesky at leseska@ccf.org.
Advertisement
Advertisement

Collaboration includes clinical validation of predictive modeling tool, development of second-generation tool

TVT Registry analysis could expand indication to lower surgical risk levels

Patient series and bench validation support efficacy and safety of CLEVE procedure

In the wake of NOTION-3 findings, a strong argument for physician judgment remains
Post hoc analysis of PROTECTED TAVR finds reduced stroke risk in the U.S. but not beyond

Analysis of STS/ACC TVT Registry finds greatest benefit in patients with prior stroke

TAVR explant demands multidisciplinary expertise
Support for a TAVR-first approach in patients with concurrent valve and coronary disease