Locations:

Large study finds seven protocols valid for predicting mortality risk
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/69de25d2-69ba-41cc-8d40-16272ee33c18/20-HVI-1917085-treadmill-stress-echo-650x450-1_jpg)
20-HVI-1917085-treadmill-stress-echo-650×450
Estimated metabolic equivalents (METs) determined by the Bruce, Cornell and Naughton standardized exercise protocols reliably predict risk of death, but results are not transferable across different tests. That’s the major takeaway from a study that examined results of more than 120,000 patients from a Cleveland Clinic stress test registry over a 25-year period. The study was published in the July 9 issue of the Journal of the American Heart Association.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Lower exercise capacity is associated with higher death rates regardless of which protocol is used,” says the study’s senior study author, Wael Jaber, MD, a Cleveland Clinic staff cardiologist. “However, not all stress tests are alike, so a patient’s MET values from consecutive exercise stress tests provide comparable information only if the same protocol was used.”
While the Bruce exercise stress test has been well validated for predicting mortality, other options are frequently used instead, particularly for patients with physical limitations that necessitate testing with a less demanding protocol. However, limited data are available on the prognostic value of the alternative tests. Furthermore, whether estimated METs obtained from different protocols are comparable has not been previously studied.
This study included exercise stress test records of patients who underwent testing at Cleveland Clinic from January 1991 through February 2015. For patients with repeat tests, only the first results were used. Data from patients who were referred for or converted to pharmacological testing were excluded.
The analyzed cohort consisted of 120,705 patients (mean age, 53.3 ± 12.5 years; 59% men). The following exercise stress protocols were represented:
The primary outcome was all-cause mortality. Data on deaths were obtained through June 10, 2016, from the Social Security Death Index and patient charts. Over mean follow-up of 8.7 years, 8,426 patients died (6.9%).
Advertisement
As the most widely used protocol in the cohort, the Bruce protocol served as the reference standard to which the other protocols were compared in terms of mortality prediction after multivariable adjustment for comorbidities, medications and estimated METs.
Graphic comparison of the protocols’ prognostic value is presented in the figure below, which highlights the following major findings:
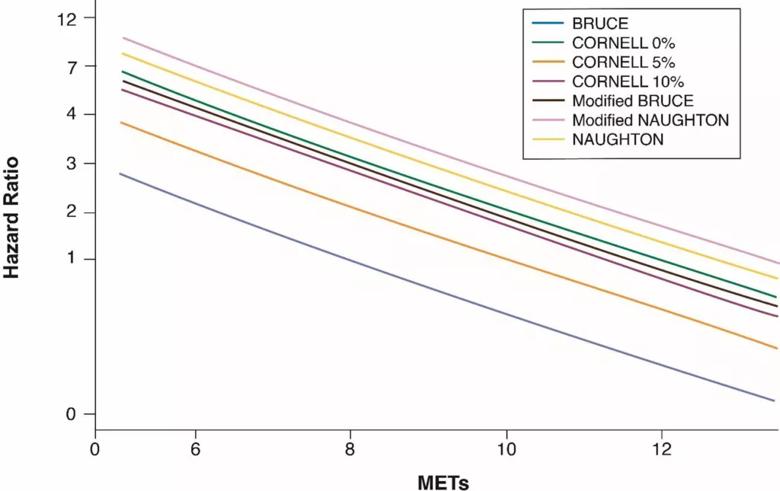
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e80456bd-7662-4c3d-9bd5-6fd90454dedc/Inset-graph-Please-just-resize-for-optimal-CQD-viewing-1024x645_png)
Figure. Association of METs with mortality across different exercise protocols. Reprinted from Harb et al., J Am Heart Assoc. 2020;9:e015986, under the Creative Commons Attribution–Noncommercial License. ©2020 The Authors.
“Interpretation of MET values must be confined within the protocol that the patient was tested with,” observes the study’s lead author, Serge Harb, MD, a Cleveland Clinic staff cardiologist. “When determining prognosis, the specific test used is as important as the METs achieved.”
An interesting finding, adds study co-author Pavan Bhat, MD, is that the non-Bruce protocols were associated with higher hazard ratios compared with the Bruce protocol despite robust risk factor adjustment. “It’s possible that factors not captured in the data registry — such as frailty or features of impairment assessed at bedside — may have been more common in patients referred for a non-Bruce protocol,” notes Dr. Bhat, a Cleveland Clinic staff cardiologist. This theory is supported by the likelihood that patients with heart failure were more often tested with the Naughton protocol than the Bruce protocol, for historical reasons.
Advertisement
The authors also point out that the 25-year duration of the study period may have introduced bias. Although median patient age generally remained stable over that time, the number of patients referred for pharmacological testing increased over the study period. This may have skewed referral patterns towards less healthy patients undergoing non-Bruce protocols.
Moreover, electrocardiographic and imaging data could shed light on differences in patient populations among the protocols but were not included in multivariable adjustments.
Most importantly, the authors note, the results may reflect an inherent weakness in metabolic exercise stress testing — specifically, limitations in how accurately estimated METs reflect exercise ability compared with peak VO2 measurements. Variability among the protocols in this regard could contribute to the observed variations in hazard ratios.
Despite these limitations, this study drew on the largest cohort of stress tests using non-Bruce protocols to date to reveal previously unknown findings with important implications, Dr. Jaber concludes. “These results, while showing the validity of the different protocols for predicting mortality, can help form the basis for protocol recalibration to improve individual accuracy as well as comparability,” he says.
Advertisement
Advertisement

New framework better distinguishes stable from critically ill patients

CMR-CLIP outperforms general AI tools; may one day expand patient access to CMR

Post hoc analysis of CLEAR Outcomes trial bolsters its case as a statin alternative

Large retrospective analysis may prompt prospective studies

How to talk about lifetime risk, treatment goals, Lp(a) testing, statin skepticism and more

A scannable recap of recent volumes and clinical metrics from Cleveland Clinic

Cleveland Clinic reports first U.S. series focused on use in this challenging setting

Large series confirms early and long-term survival advantages over partial pericardial resection