Locations:

Fully-automated process uses preop CT, baseline GFR to estimate post-nephrectomy renal function
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/c67eadb0-a470-4e95-9f8f-8d9c94a59e6c/normal-glomerulus)
Drawing of a pink bulb with two tubes coming out of the top
An artificial intelligence (AI)-generated calculation of glomerular filtration rate (GFR) is as accurate as a validated clinical model for predicting renal function after partial or radical nephrectomy. So says a study by Cleveland Clinic investigators that was recently presented at the International Kidney Cancer Symposium: North America and cited as an award-winning poster.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“This is the first fully-automated model that clinicians can potentially use to predict post-op GFR at the point of care with no human input from the preoperative CT scan,” says Christopher Weight, MD, Director of the Center for Urologic Oncology at Cleveland Clinic. “Our research shows that it is accurate not only for calculating value but also for determining whether GFR is likely to fall below the level where the American Urological Association recommends prioritizing partial over radical nephrectomy.”
This retrospective study included 300 patients undergoing partial or radical nephrectomy from the 2021 Kidney and Kidney Tumor Segmentation challenge (KiTS21). In KiTS21, teams around the world competed to develop the best system for automatic semantic segmentation of renal tumors and surrounding anatomy. Seven of the patients ultimately were excluded because their tumors were bilateral.
“Although this was a single-center study in terms of the surgery, the CT scans we used from KiTS21 were performed at 70 different medical facilities, which supports the potential generalizability of our findings,” says Nour Abdallah, MD, a urologic oncology research fellow at Cleveland Clinic and first author of the study.
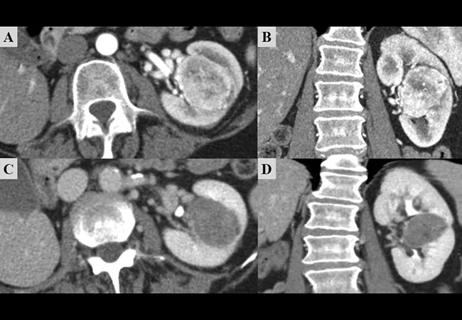
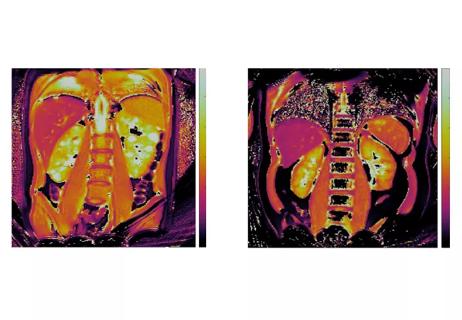
Split renal function (SRF) was determined based on preoperative CT scans and a deep-learning segmentation model. Preoperative GFR was defined as the last recorded value before a patient’s surgery. Postoperative GFR was defined as the value measured 90 or more days following the procedure.
Advertisement
The authors programmed the AI algorithm to estimate postoperative GFR based on the following equation: 1.24 × preop GFR × contralateral SRF for radical nephrectomy or 89% of preoperative GFR for partial nephrectomy.
The clinical model used, which was previously validated in a cohort of more than 3,000 patients from Cleveland Clinic, was the baseline estimated GFR (NB-GFR) formula: GFR = 35 + preoperative GFR (× 0.65) - 18 (if radical nephrectomy) - age (× 0.25) + 3 (if tumor size > 7 cm) - 2 (if diabetes).
To compare the accuracy of the AI algorithm and clinical model GFR estimates, the researchers used correlation coefficients. Logistic regression and area under the curve (AUC) calculations were performed to determine comparability of the two methods in predicting which patients would have a postoperative GFR < 45 mL/min/1.73 m2.
The median age of the 293 patients enrolled was 60 years; 40.6% were female and 62.1% had undergone partial nephrectomy. Median body mass index was 29.7 kg/m2 and 19.8% of the patients had diabetes.
Among the cohort, median size of tumors was 4.2 cm, the majority (91.8%) of which were malignant. Of those masses, 35.1% were high grade, 25.6% were high stage and 21.8% had necrosis.
The correlation coefficients for postoperative GFR measurement were 0.75 for the AI algorithm and 0.77 for the validated clinical model. The AUCs for prediction of postoperative GFR < 45 mL/min/1.73 m2 were 0.89 for the AI algorithm and 0.90 for the validated clinical model.
Advertisement
“The area under the curve for the AI algorithm was almost identical to the clinical model,” says Dr. Weight, noting that the clinical model is time-consuming for urologists to use and, therefore, not widely adopted. “This indicates that AI, which can be completely automated, is a much simpler and faster method, and is as accurate a way to predict post-op GFR as a previously validated clinical model.”
The next step for the researchers — and one that is already underway — is validation of their results in a much larger cohort.
“In the meantime,” says Dr. Abdallah, “we hope that our results will encourage clinicians to get beyond thinking that AI is a ‘black box’ and embrace the idea that it can be very useful in the management of kidney cancer.”
Advertisement
Advertisement

One pediatric urologist’s quest to improve the status quo

First single-port renal vein transposition reduces recovery time and improves outcomes
Belzutifan superior to everolimus in phase 3 clinical trial
Management of high-risk RMSK in the pre-and current eras of neoadjuvant therapy
NIH-funded study explores novel MRI technique to stage cystic kidney disease

AI-generated model bests predictive abilities of human experts
Study highlights benefits of nephrologist-led urine sediment analysis

Using sequencing data to identify novel factors linked to kidney disease with unknown origin