Locations:

Physio-VT study results are likely to shift practice in mapping and ablation of VT
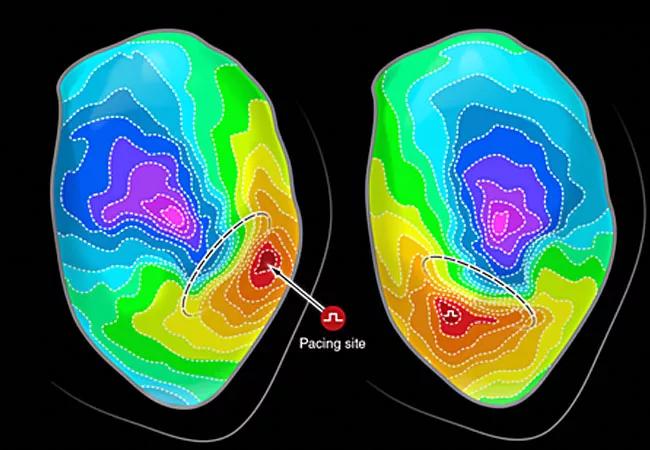
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/420202c3-82d0-4a1f-834b-1196116da33d/20-HVI-1886651-ablation-mapping-650x450-1_jpg)
20-HVI-1886651-ablation-mapping-650×450
A novel method for mapping and ablation in patients with scar-related ventricular tachycardia (VT) may improve the clinical outcomes of VT ablation procedures, report investigators with the international multicenter Physio-VT study. Results of the study were presented virtually this week during the Annual Scientific Sessions of the Heart Rhythm Society and simultaneously published in Circulation: Arrhythmia and Electrophysiology.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The core of this new methodology is mapping of the heart during activation from multiple directions, in contrast to the standard technique of mapping the heart from only a single direction. “The additional information obtained from mapping the heart during activation from multiple directions (and potentially cycle lengths) increases the sensitivity and specificity of mapping, which can then be used for identifying the underlying arrhythmogenic substrate,” says the study’s principal investigator, Elad Anter, MD, Associate Section Head of Cardiac Electrophysiology at Cleveland Clinic and Director of its VT Program.
The clinical outcome of ablation in patients with scar-related VT has traditionally been disappointing, with recurrence rates of 30% to 40% within two years. “The major limitation of ablation is the insufficient mapping specificity for identifying, and then targeting with ablation, the true arrhythmogenic substrate responsible for VT,” Dr. Anter explains.
He notes that standard methods used for mapping and ablation of VT are flawed as a result of assumptions and misconceptions. “One of these misconceptions is that scar equals arrhythmia, and therefore should be the target of ablation,” Dr. Anter says. “However, this is often not the case. The majority of patients with a history of myocardial infarction never develop VTs, and even in those who do, only part of the infarct (not the whole infarct) is responsible for development of VT.”
The focus of Dr. Anter’s research laboratory and clinical practice is the study of the mechanisms of arrhythmias and development of new technologies that can improve the specificity of identifying the arrhythmogenic substrate responsible for VT.
Advertisement
The Physio-VT study was based on preclinical studies performed in Dr. Anter’s research lab as well as in the lab of Dr. Andrew Wit, an emeritus professor of pharmacology at Columbia University in New York and a co-investigator in the Physio-VT study. They found that VT circuits in healed infarctions often colocalize to sites exhibiting activation slowing during sinus rhythm. However, in order to identify the full extent of the circuit and all potential circuits, LV activation from multiple directions is often required.
Physio-VT is an international, prospective, single-arm study of 85 patients with infarct-related VT that was refractory to antiarrhythmic medications, with a substantial fraction having failed previous ablation procedures. In these patients, mapping of the left ventricle (LV) was performed using high-resolution technologies and activation from multiple directions, including sinus rhythm, right ventricular and left ventricular pacing at a constant cycle length of 600 milliseconds. For each activation wavefront, the area of maximal activation slowing was marked and targeted for ablation. Patients were followed a median duration of 3.6 years, and the study’s primary endpoint was a composite of appropriate ICD therapies and cardiovascular death.
The study showed that in comparison to standard LV mapping during activation from a single direction, LV activation from multiple directions identified an additional ~30% of areas exhibiting slow activations that were responsible for an additional 25% of VT circuits that could not be identified during activation from a single direction. During the follow-up period, only 16.5% of patients had VT recurrence, a significantly lower incidence compared with results from the published literature (Figure).
Advertisement
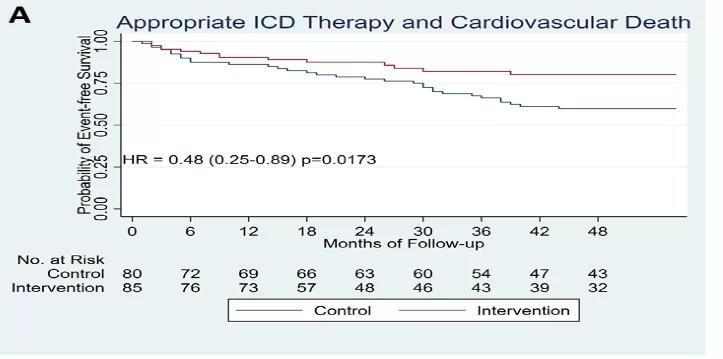
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/61c41489-fc43-43e8-a5af-53312c6db6a5/20-HVI-1886660-Inset-1_png)
Figure. Comparative clinical outcomes between the novel ablation method in Physio-VT (intervention) and a historical control group ablated using standard mapping methods.
“The important physiological observations made by this pivotal study, as well as the remarkable clinical outcomes, are highly encouraging and may represent a paradigm shift in treatment of VT,” says Oussama Wazni, MD, Section Head of Cardiac Electrophysiology at Cleveland Clinic. “The results of this study demonstrate that diligent, physiologically driven mapping strategies may have a positive impact on catheter ablation for VT as well as the entire field of electrophysiology.”
The next step, Dr. Anter says, is a randomized controlled study led by Cleveland Clinic to validate these findings.
Advertisement
Advertisement

Innovative approach to living-tissue AVR achieves low reintervention rates, excellent long-term survival

Diagnosis and treatment of malnutrition and cachexia are key to improving cardiac outcomes

Symptom burden at presentation is a potent predictor of long-term survival, large analysis shows

New framework better distinguishes stable from critically ill patients

CMR-CLIP outperforms general AI tools; may one day expand patient access to CMR

Post hoc analysis of CLEAR Outcomes trial bolsters its case as a statin alternative

Large retrospective analysis may prompt prospective studies

How to talk about lifetime risk, treatment goals, Lp(a) testing, statin skepticism and more