Locations:

Nodule removal avoids need for exenteration
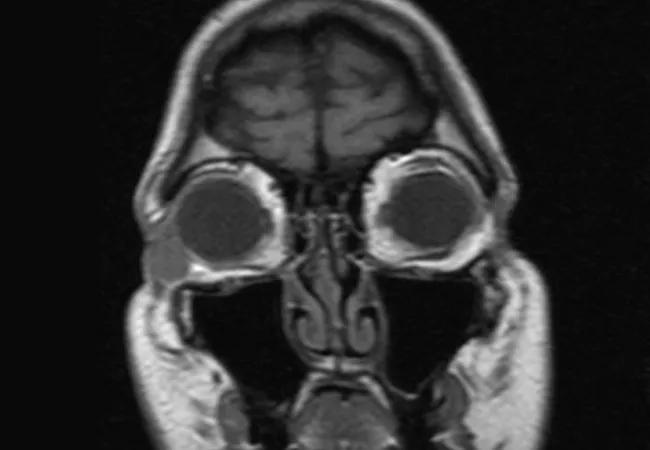
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/1f869897-613f-432b-8dc6-6e268d4d497c/18-EYE-4340-A-Singh-CQD-Hero_jpg)
Orbital Nodular Fasciitis in an Adult Misdiagnosed as Sarcoma
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Nodular fasciitis is a reactive fibroblastic growth arising from subcutaneous or superficial fascia. Commonly presenting as a rapidly growing mass in the trunk or extremities, nodular fasciitis rarely presents in the periorbital tissues. Herein, we report the case of a 51-year-old man with nodular fasciitis of the inferolateral orbit, which was initially misdiagnosed as sarcoma.
A 51-year-old male was referred to ocular oncology clinic at the Cole Eye Institute for exenteration for a rapidly enlarging right lower orbital mass of two months’ duration. His medical history was significant for non-Hodgkin’s mantle cell lymphoma two years prior to presentation, for which he had received chemotherapy and subsequent bone marrow transplant.
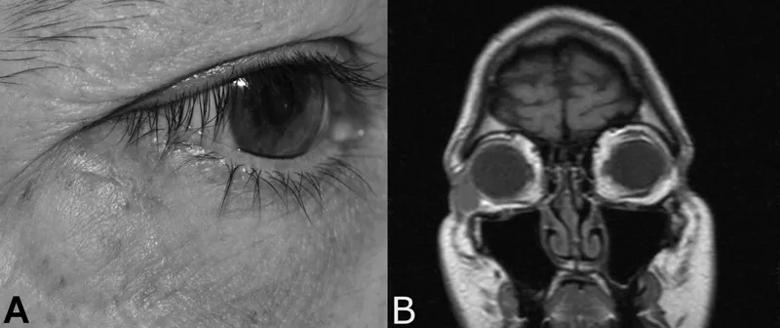
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/2cdeefea-a949-4dee-bea8-05144b770aee/18-EYE-4340-A-Singh-CQD-Inset-1_jpg)
Figure 1: A. External photograph showing inferotemporal orbital nodule
B. T1 weighted coronal MRI showing well-circumscribed nodule in the inferotemporal orbit, which is isointense to muscle
Initial evaluation and incisional biopsy at an outside hospital led to the diagnosis of a pleomorphic undifferentiated sarcoma. A 2.2 cm x 2.5 cm round, hard mass was palpated at the inferolateral orbit that was adherent to underlying tissues and separate from the overlying skin (Figure 1A). Proptosis and abnormal extraocular movements were absent. There were no signs of optic disc compression. Orbital magnetic resonance imaging with gadolinium showed a 1.7 cm x 1.0 cm x 1.4 cm homogeneously enhancing subcutaneous mass in the right inferolateral orbit, which was hyperintense on T2 and isointense to muscle on T1, with mild diffusion restriction (Figure 1B). The mass was localized to the preseptal tissues without invasion of the globe, muscles or bone.
Advertisement
Given the ramifications of exenteration and the well-circumscribed appearance of the mass on imaging, a decision was made to undertake excisional biopsy, accepting the possibility of microscopic residual disease to be treated by radiation therapy and chemotherapy. The patient underwent anterior orbitotomy with excision of the mass in its capsule. Intraoperatively, the mass was noted to be free from rectus muscle or sclera, but was adherent to the inferolateral periosteum, which was removed with the capsule.
The patient did well post-excision with no evidence of recurrence.
Hematoxylin and eosin stained sections showed a well-marginated proliferation of cytologically bland spindle cells arranged in short fascicles with intermixed osteoclast-like giant cells and extravasated red blood cells (Figure 2A/B). Nuclei were uniform without significant atypia. Scattered mitotic figures were noted, but there were no atypical mitotic forms. Immunohistochemical stains showed the spindle cells to be positive for smooth muscle actin (Figure 2C) and negative for STAT6 and desmin. Taken together, these findings were most consistent with nodular fasciitis.
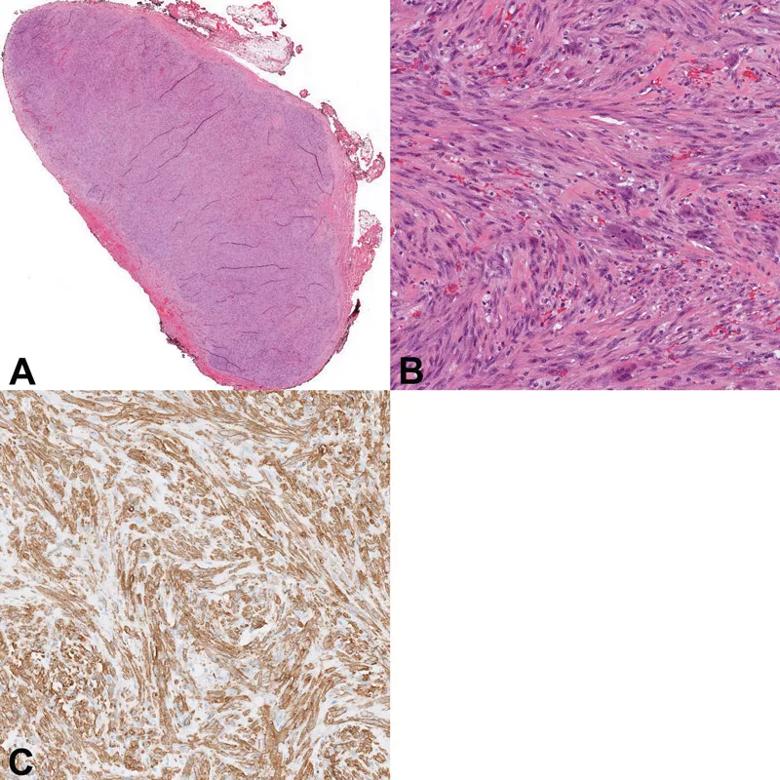
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/020ed6b5-994d-4572-b0fd-d113e392beff/18-EYE-4340-A-Singh-CQD-Inset-2_jpg)
Figure 2: A. Hematoxylin and eosin stained section of well-circumscribed nodule in its capsule
B. Higher magnification hematoxylin and eosin stained section showing spindle cells arranged in short fascicles and scattered red blood cells
C. Spindle cells stained highly positive with smooth muscle actin
Nodular fasciitis is a reactive fibroproliferative growth that arises from the subcutaneous and superficial fascia. Typically found in the trunk and extremities, nodular fasciitis rarely presents in the ocular and periorbital tissues. In all, nodular fasciitis has been reported in the orbit, the eyelid, the periorbita and the epibulbar tissues. To the authors’ knowledge, 11 cases of nodular fasciitis in the orbit have been reported, with only three being in adults. The pathophysiology of nodular fasciitis is debated; previous reports have postulated that it is a reactive process to repetitive trauma. Discovery of a recurrent USP6 gene rearrangement in nodular fasciitis, however, suggests that it may be a transient neoplastic process.
Advertisement
Nodular fasciitis often presents as a rapidly growing mass that can be difficult to distinguish from malignant sarcoma clinically and histologically. Histopathology typically shows hypercellularity with spindle shaped fibroblasts in a myxoid matrix, with scattered mitotic figures but no atypia. Fine needle aspiration biopsy has been explored as a less invasive method for diagnosing nodular fasciitis, but has proven difficult. In a sample of 34 fine needle aspiration biopsies of nodular fasciitis, only 4 cases were interpreted as nodular fasciitis, only 6 cases as definitively benign, and two cases were interpreted as malignant neoplasm. In this case, incisional biopsy prior to presentation was interpreted as pleomorphic undifferentiated sarcoma, for which definitive treatment (ie. exenteration) would have been unnecessarily invasive and morbid. New molecular markers such as USP6 gene rearrangements, reported in 92% of cases in one series, may be useful to differentiate nodular fasciitis from malignant entities such as fibrosarcoma and enable less invasive treatment in the future.
Surgical excision with pathology is the definitive diagnosis and treatment for nodular fasciitis. Recurrence after complete excision is rare; in a series of 272 cases of nodular fasciitis in China, only one recurred post-excision. Recurrence rates in ocular and orbital nodular fasciitis post-excision have not been examined, in part due to its rare presentation in these locations. Notably, however, there were no recurrences in the eleven previously reported cases of orbital nodular fasciitis, despite incomplete excision in two of these cases.
Advertisement
In conclusion, we present the case of a 51-year-old man with orbital nodular fasciitis, highlighting this rare entity and the importance of differentiating it from similar malignant mimics.
Rachel C. Chen, MD, Jose J. Echegaray, MD, Ryan S. Berry, MD, and John Goldblum, MD, contributed to this article.
Advertisement
Advertisement

The drug does not provide lasting disease control for most patients

New service for patients with diabetes will make annual screening more convenient

Gonioscopy can help determine next steps in reducing IOP

Similarly, patients with noninfectious uveitis have a higher risk of being diagnosed with an autoimmune disease within five years

A review of pathophysiology, risk factors, clinical presentation and treatment options

How computational tools and personalized biomechanics can improve keratoconus detection, ectasia risk assessment and surgical outcomes

Motion-tracking Brillouin microscopy pinpoints corneal weakness in the anterior stroma

Registry data highlight visual gains in patients with legal blindness