Locations:

A case report
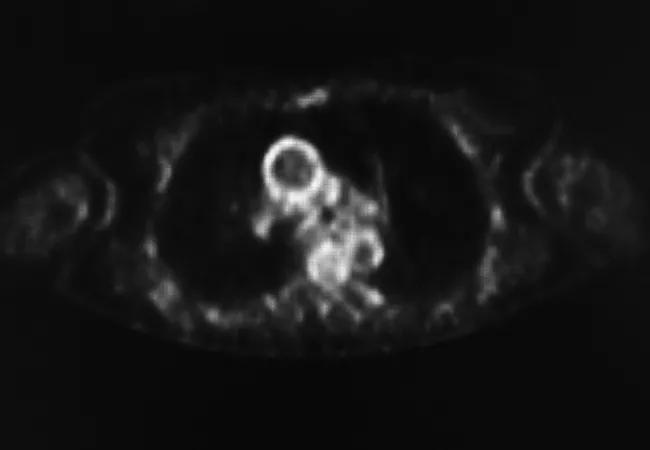
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/bd5f5b1f-db53-46af-8767-759130d64195/18-RHE-1027-Langford-Hero-Image-650x450pxl_jpg)
18-RHE-1027-Langford-Hero-Image-650x450pxl
By Kevin Byram, MD, Carol A. Langford, MD, MHS
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 49-year-old male was diagnosed with Takayasu arteritis (TAK) three years ago. At that time, he presented with headache and was found to have severe hypertension and an absent left radial pulse. His sedimentation rate (ESR) and C-reactive protein (CRP) were elevated, and he had normal renal function. Vascular imaging revealed a stenotic left subclavian artery and an occluded left renal artery with an atrophic left kidney. Following his diagnosis, he was started on glucocorticoids and methotrexate, with medical management of his hypertension. He initially did well, but recent laboratory evaluation revealed mild elevations in his ESR and CRP. He was having no new symptoms and his physical examination was stable, including four-limb blood pressures and bruit evaluation. He had recently read about positron emission tomography (PET) imaging and had questions about its clinical utility.
Giant cell arteritis (GCA) and TAK are the two most common forms of primary large vessel vasculitis (LVV). Assessment of disease activity in patients with LVV is an ongoing challenge. Currently, the clinician integrates information from the history, physical examination, laboratory and available imaging to reach a conclusion regarding ongoing inflammatory disease activity.
From an imaging standpoint, computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are the main modalities used to assess the vascular lumen in patients with LVV. Detection of a new stenosis or aneurysm on serial imaging is usually considered to be indicative of disease activity necessitating treatment. However, once these lesions develop, vascular damage has already occurred, such that there is interest in techniques that could identify vascular inflammation prior to the development of a stenosis or aneurysm in patients with LVV.
Advertisement
Position emission tomography (PET) is a mode of imaging utilizing 18F-fluorodeoxyglucose (FDG) uptake to determine the metabolic demands on various body tissues. Hypermetabolic tissues will demonstrate increased FDG uptake on PET scans potentially providing insights into the biological processes occurring at a particular site of interest.
The established clinical indication of FDG-PET is for the assessment of oncological diseases. The use of FDG-PET in inflammatory diseases is a subject of ongoing investigation. In LVV, the unique metabolic mechanism of PET imaging has raised interest in whether it could provide a means for clinicians to identify vascular inflammation and “pre-structural” disease activity.
A large prospective, observational study was recently conducted at the National Institutes of Health (NIH) to characterize the role of PET imaging as a biomarker in patients with LVV. The study enrolled 67 patients with GCA and 44 with TAK with a comparator group comprised of healthy controls (n = 7), patients with hyperlipidemia (n = 35), and patients with disease mimicking LVV (n = 7).
Prior to and independent of imaging studies, disease activity was determined by clinical history, physical examination and laboratory assessment. FDG-PET was performed at baseline and at each follow-up visit. PET studies were examined by nuclear radiologists and determined dichotomously to be positive for vasculitis and negative for vasculitis. A novel assessment tool defined in this study was the PET Vascular Activity Score (PETVAS), a semi-quantitative score rating PET uptake intensity relative to the liver on a 0-to-3 scale in nine vascular territories (0 = no FDG uptake, 1 = less than liver, 2 = equal to liver, 3 = more than liver).
Advertisement
In this study, FDG-PET had a sensitivity of 85 percent and specificity of 83 percent when differentiating active LVV from comparator groups. The sensitivity dropped to 42 percent when differentiating active LVV from those patients with LVV in remission. Some patients with LVV who were in clinical remission maintained persistent FDG uptake signal on follow up PET scans. The researchers also found an association between relapse risk and PETVAS score in which more patients who had a PETVAS greater than or equal to 20 relapsed compared to those with PETVAS less than 20 (45 vs 11 percent, P = 0.03).
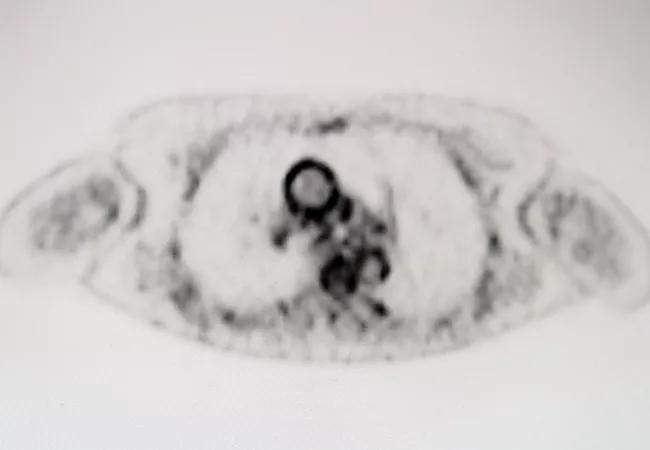
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/187771dc-e84d-4053-82a1-4cde2349b8a2/18-RHE-1027-Langford-Inset-Image-650pxl-width_jpg)
Axial FDG-PET images from a patient with aortitis demonstrating increased FDG uptake in the aortic root and ascending aorta.
The role of PET imaging in patients with LVV has yet to be clearly defined. In the NIH study, although FDG-PET demonstrated reasonable ability to discriminate patients with active LVV from other disease settings and healthy controls, FDG uptake was also seen in some patients with atherosclerosis and other mimicking disease processes. FDG-PET did not reliably differentiate patients with active LVV from those in remission, and more studies are needed to better understand whether persistent PET uptake represents increased metabolic activity from vascular remodeling or subclinical active inflammation.
A key issue that remains is whether FDG-PET characteristics, such as PET uptake and PETVAS score, correlate with the later development of structural arterial consequences, such as a new stenosis or aneurysm. Longer-term, serial follow-up from the NIH and other cohorts may provide answers to this important question in this complex patient population.
Advertisement
Until there are more definitive answers regarding the utility of FDG-PET in LVV, the decision about whether to pursue such imaging should be made on an individual basis. Factors to weigh include the specific question being asked and the currently available evidence, as well as cost and access issues. If PET is performed, this information should be used adjunctively with CTA or MRA, as these methods of imaging remain critical in order to assess vascular anatomy.
To assess the disease activity of our patient with TAK, we recommended MRA of the entire aorta and branch vessels, which did not reveal any new vascular lesions. While slightly elevated, his inflammatory markers were at his baseline. Given no new symptoms, stable labs and unchanged vascular lumen imaging, he was deemed to be in clinical remission and no changes were made to his medical regimen. In the six-month interim, he is still in clinical remission. In the absence of new symptoms or signs, we will plan to repeat his MRA every 12 months.
Dr. Byram is completing a one-year vasculitis fellowship in Cleveland Clinic’s Center for Vasculitis Care and Research. His fellowship has been supported by the Vasculitis Clinical Research Consortium (VCRC), the Vasculitis Foundation and Vanderbilt University Medical Center, where he will be returning following his fellowship.
Dr. Langford is Director of the Center for Vasculitis Care and Research as well as Vice Chair for Research, Department of Rheumatic and Immunologic Diseases.
Advertisement
Advertisement

Researching the biological basis for why treatment is or is not effective

Scribing system helps create more face-to-face interactions

A conversation with Leonard Calabrese, DO

The case for continued vigilance, counseling and antivirals

High fevers, diffuse rashes pointed to an unexpected diagnosis

No-cost learning and CME credit are part of this webcast series

Summit broadens understanding of new therapies and disease management

Program empowers users with PsA to take charge of their mental well being