Locations:

Largest U.S. study of extended repair of acute DeBakey type I dissection
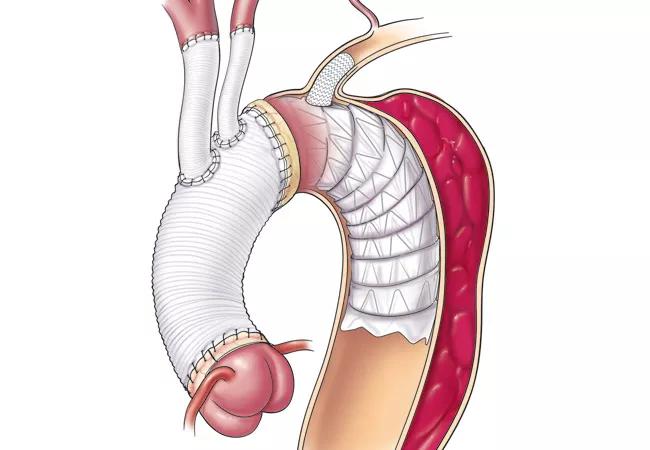
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/edb54288-dd32-42fc-9bb9-0766536d0a09/18-HRT-310_Elephant-trunk-Hero_jpg)
18-HRT-310_Elephant trunk-Hero
Despite encouraging results elsewhere, uptake of frozen elephant trunk repair for acute DeBakey type I dissection has been slow in the United States. A new report of midterm outcomes with the procedure at Cleveland Clinic could help change that by demonstrating that a simplified approach to the technique is safe, promotes aortic remodeling and eases management of chronic aortic complications.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“Our experience shows that, at centers of excellence, frozen elephant trunk repair can be performed with mortality comparable to the conventional hemiarch repair strategy even in patients who present with ischemia,” says Cleveland Clinic cardiothoracic surgeon Eric Roselli, MD, lead author of the report, published as the cover feature of the March 2018 issue of Annals of Thoracic Surgery.
The traditional approach to acute DeBakey type I dissection has been conservative, limiting repair to replacement of the ascending aorta and hemiarch. But recent years have seen refinement of operative techniques and the emergence of endovascular devices that make an extended initial repair possible with acceptable risk.
“At Cleveland Clinic, we’ve developed a simplified hybrid approach involving single anastomosis frozen elephant trunk repair,” explains Dr. Roselli, Surgical Director of Cleveland Clinic’s Aorta Center. “Since we published our initial experience with this technique in 2013, we have refined the procedure to improve effectiveness and further disseminate its use.”
That refinement and the resulting outcomes are the focus of his team’s new report, which profiles the management of 72 patients with DeBakey type I dissection who underwent emergency simplified elephant trunk repair at Cleveland Clinic from 2009 to 2016.
The most common presentation was aortic insufficiency, followed by malperfusion, followed by rupture. Concomitant procedures included valve resuspension, root replacement, cusp repair and valve replacement. The first 39 patients were treated with modification of an early-generation stent graft, the next 16 patients received newer modified stent grafts, and the 17 most recent patients underwent the branched single anastomosis frozen elephant trunk repair (B-SAFER) technique with left subclavian stent grafting.
Advertisement
Primary outcomes in the study report were operative mortality and neurologic complications, including stroke and spinal cord injury.
Operative mortality was 4.2 percent (3 of 72 patients): Two patients were comatose at presentation without recovering, and the other died from coagulopathy complications.
Morbidity included the following:
Over median follow-up of 28 ± 25 months, survival was as follows:
Among the 63 surviving patients with follow-up imaging available, 92 percent demonstrated thrombosis in the false lumen of the treated segment. Complete reverse remodeling with shrinkage of the false lumen was seen in 54 percent of patients, with the mean total aortic diameter reduced from 42 ± 8 mm to 37 ± 7 mm.
Ten patients required 14 late reinterventions for aortic growth and progression of their dissection disease. Freedom from reintervention was as follows:
“Our midterm outcomes show that the simplified frozen elephant trunk technique promotes false lumen thrombosis and reverse remodeling of the aorta in the treated segment,” says Dr. Roselli. “Our modified single anastomosis strategy has maintained relatively low circulatory arrest times and has enabled wider use among our team of surgeons.”
Advertisement
He notes that he and his colleagues tailor their approach to acute ascending aortic dissection according to the aortic pathology, presentation and patient characteristics. “A minimally invasive approach with ascending TEVAR is reserved for exceptionally high-risk patients who aren’t candidates for open repair,” he adds.
In an invited commentary accompanying the report, T. Brett Reece, MD, of the University of Colorado notes that while only further follow-up will determine whether this technique will ultimately prevent late aortic reintervention, “the authors should be lauded for their perseverance and follow-up of these complex patients.”
Dr. Reece concludes as follows: “We are quickly approaching more complete replacements of the arch to not only allow patients to fight another day, but also with the ultimate goal of fighting independent of the need for further aortic intervention.”
Advertisement
Advertisement

‘Sac flow’ is more precise and will ease unfounded patient concerns, experts argue

Join us in New York Dec. 4-5 for evidence-based instruction with real-world examples

First-ever transcarotid artery revascularization trial with no strokes or device-related deaths

Consensus statement outlines the team, infrastructure and experience needed to deliver TTVI safely and effectively

Innovative approach to living-tissue AVR achieves low reintervention rates, excellent long-term survival

Diagnosis and treatment of malnutrition and cachexia are key to improving cardiac outcomes

Symptom burden at presentation is a potent predictor of long-term survival, large analysis shows

New framework better distinguishes stable from critically ill patients