Locations:

Data-driven segmentation approach shows promise for seizure characterization with utility for clinical decision making
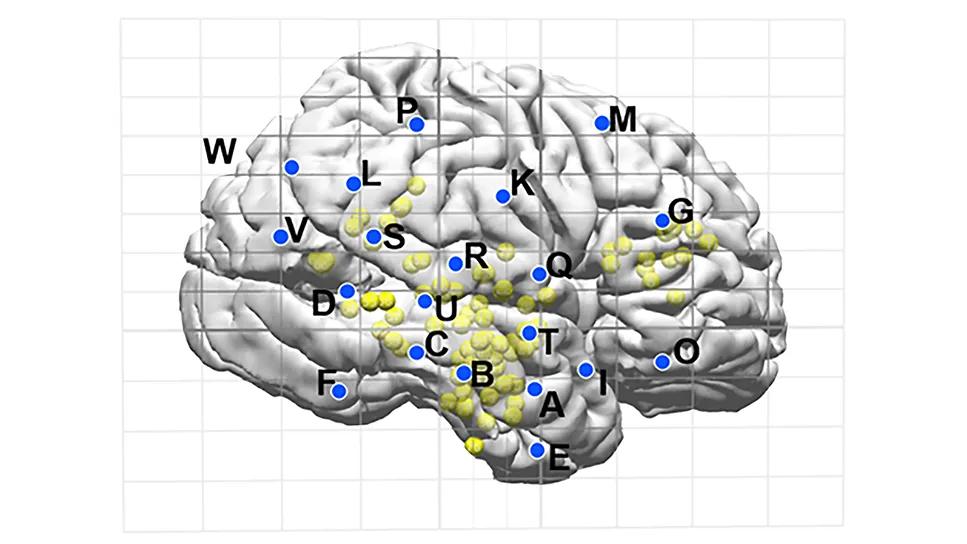
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/ea57ad06-e088-48e9-a080-e3710d4a9960/learnings-from-1000-seegs)
brain illustration covered with dots and letter labels atop a ruled grid
For patients with drug-resistant focal epilepsy, the success of surgical intervention rests on precise localization of the seizure onset zone. While stereoelectroencephalography (SEEG) has revolutionized the ability to record from deep cortical structures with millimeter precision, the sheer volume of data produced during invasive monitoring remains a challenge. Traditionally, clinicians have relied on time-intensive visual inspection to identify not just when a seizure starts, but how it transforms and spreads — a process often hindered by subjectivity and significant variability among experts.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A new Cleveland Clinic study published in the Annals of Biomedical Engineering introduces a potential paradigm shift: a semi-supervised, automated framework capable of segmenting seizures into three distinct physiological phases with a degree of accuracy that rivals the judgment of experienced epileptologists. By identifying seizure onset, internal transitions and termination, this tool — which the researchers call a changepoint detection framework — offers an objective, reproducible roadmap of seizure dynamics that could significantly streamline presurgical evaluations.
The concept of “seizure detection” is often treated as a binary — i.e., a seizure is either happening or it isn’t. However, clinicians know that a seizure is a dynamic, evolving event. It progresses through stages of initiation, propagation across networks and eventual cessation. Identifying these internal intra-ictal transitions is critical because they mark the moments when a seizure recruits new brain regions.
Understanding this temporal evolution is what allows a surgical team to distinguish the true zone of origin from areas that are merely involved in secondary spread. Unfortunately, while automated tools have become quite good at flagging the presence of a seizure, they have historically fallen short in providing precise temporal boundaries — the “changepoints” — that clinicians need to map these complex propagation patterns.
The Cleveland Clinic research team, led by Balu Krishnan, PhD, developed a pipeline that uses a multivariate changepoint detection algorithm known as PELT (Pruned Exact Linear Time). Rather than looking at a single aspect of the EEG, the system tracks seven different characteristics of the electrical signal simultaneously: amplitude; relative power across the theta, alpha, beta and gamma frequency bands; spectral entropy; and a measure of cumulative signal complexity called line length.
Advertisement
The study analyzed 179 onset-zone bipolar channels across 32 seizures recorded in 10 patients with drug-resistant focal epilepsy who were successfully treated with surgery at Cleveland Clinic. Because these patients achieved seizure freedom after their procedures, the electrode contacts identified as being in the seizure onset zone provided a gold standard for testing the algorithm.
The researchers designed the system to be “length-invariant,” meaning it can accurately find seizure boundaries regardless of the amount of pre-ictal or post-ictal data captured in the recording. “This ensures the algorithm is learning true neural dynamics rather than just looking for a change at a fixed point in time,” Dr. Krishnan explains.
The framework was tasked with identifying three specific milestones: the earliest ictal onset, the most significant transition during the seizure and the final termination point. The results demonstrated a high level of temporal precision:
For context, the researchers noted that these error margins are within the typical range of disagreement between two different human experts looking at the same data. In terms of practical accuracy, the system correctly identified onset and termination within a 5-second window in more than 70% of cases.
Advertisement
The study also revealed that different signal features become more or less important as a seizure progresses. At onset, high-frequency beta, alpha and gamma rhythms were the strongest markers of activity. As the seizure evolved, signal amplitude, beta power, line length and low-frequency theta power dominated, reflecting recruitment of wider networks. At termination, amplitude and line length loomed large as the most reliable indicators that the event had ended.
For clinicians, the implications of this tool extend beyond mere efficiency:
Advertisement
While the results are encouraging, the authors acknowledge certain limitations. The current study focused primarily on patients with temporal lobe epilepsy, and future work will need to validate these findings across a broader range of epilepsy syndromes. Additionally, while the system performed exceptionally well on channels within the seizure onset zone, further testing is required to see how it handles noise or artifacts in channels further away from the focal point.
“This research moves us closer to a future where SEEG analysis is more fully a high-precision science,” Dr. Krishnan concludes. “By providing an automated, expert-level assessment of seizure phases, this framework offers a powerful new lens for understanding — and more effectively treating — drug-resistant epilepsy.”
Advertisement
Advertisement

Early identification of temporal encephaloceles can improve surgical decision-making

Insights from one of the first studies of invasive monitoring in the rare form of focal cortical dysplasia

Novel Cleveland Clinic project is fueled by a $1 million NIH grant

Patients with epilepsy should be screened for sleep issues

Sustained remission of seizures and neurocognitive dysfunction subsequently maintained with cannabidiol monotherapy

Model relies on analysis of peri-ictal scalp EEG data, promising wide applicability

Investigational gene approaches offer hope for a therapeutically challenging condition
Study combines intracranial electrophysiology and SPECT to elucidate the role of hypoperfusion