Locations:

Early identification of temporal encephaloceles can improve surgical decision-making
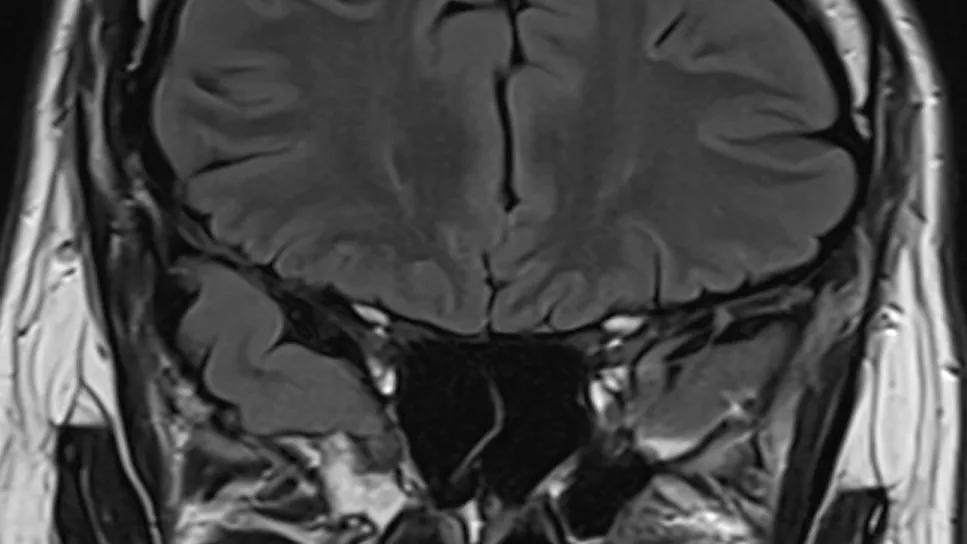
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/92f3b264-d7c0-43a7-9683-685833fa76dc/brain-mri-temporal-lobe-encephaloceles)
brain MRI taken from the back of the head
For clinicians managing drug-resistant temporal lobe epilepsy (TLE), identifying a clear structural cause is often the difference between a successful surgical outcome and ongoing seizures. A new study from Cleveland Clinic, published in Epilepsia (2025 Epub 22 Dec), introduces two novel MRI metrics — the frontotemporal aperture and the opercular angle — that significantly improve the detection of rare epileptogenic lesions known as temporal encephaloceles. The findings suggest a new mechanical theory of epileptogenesis — temporal lobe tethering.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
“We found that asymmetrical widening of the Sylvian fissure may be a hidden marker for an encephalocele, even when the lesion itself is too small to be seen on standard T1-weighted sequences,” explains Demitre Serletis, MD, PhD, a neurosurgeon in Cleveland Clinic’s Epilepsy Center who shared senior authorship of the study report with epileptologist Juan Bulacio, MD. “By applying these standardized metrics, clinicians can better identify candidates for epilepsy surgery, potentially reducing the need for invasive stereoelectroencephalography (SEEG) and improving the chances of postoperative seizure freedom.”
Temporal encephaloceles are herniations of brain tissue through defects in the skull base, typically in the middle cranial fossa. While advances in imaging have improved their discovery, they remain notoriously difficult to diagnose. Previous research indicates that even experienced neuroradiologists may miss these lesions in approximately 40% to 60% of cases.
This diagnostic gap is clinically important. Patients in the cohort of this Cleveland Clinic study — all of whom had refractory temporal lobe epilepsy and a temporal encephalocele — typically experienced epilepsy onset in their mid-20s but waited an average of 17 years before undergoing surgery. Such an interval is not unusual for patients with temporal encephaloceles, during which time these patients are often classified as having MRI-negative epilepsy, which can complicate surgical decision-making and lead to more extensive invasive monitoring.
Advertisement
For the study, Epilepsy Center researchers retrospectively analyzed 31 patients with surgically confirmed temporal encephaloceles treated at Cleveland Clinic between 2016 and 2024. To ensure consistency across different head shapes and sizes, the investigators used the Talairach referential system to measure the regional anatomy.
The study focused on two primary indices recorded on coronal MRI:
Measurements were compared between the epileptogenic side (ipsilateral to the encephalocele) and the healthy contralateral side. To ensure these metrics were specific to encephaloceles, the researchers also analyzed a control group of 14 patients with unilateral mesial temporal sclerosis.
The results revealed a distinct imaging signature for encephaloceles. Specifically, the frontotemporal aperture was significantly wider on the side containing the lesion, particularly at the anterior edge of the temporal lobe. Moreover, the temporal opercular angle was significantly smaller on the affected side, creating a wider overall opercular angle difference.
Notably, these metrics remained significant even in the 26% of patients whose encephaloceles were missed during the initial preoperative MRI review. In contrast, the control group with mesial temporal sclerosis showed no significant asymmetries in frontotemporal aperture or opercular angle, suggesting that these changes are unique to the structural distortions caused by encephaloceles.
Advertisement
These findings support what the study authors call the tethering hypothesis. Surgeons often observe that the encephalocele acts as a physical anchor; even after the lateral cortex is disconnected, the brain tissue to be resected remains attached to the skull base until the lesion is released. The widened Sylvian fissure observed on MRI likely reflects the chronic rotational or traction forces exerted on the temporal lobe by this attachment point.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4149699f-8524-40aa-aaa7-22034576917e/brain-mri-temporal-lobe-encephaloceles-inset)
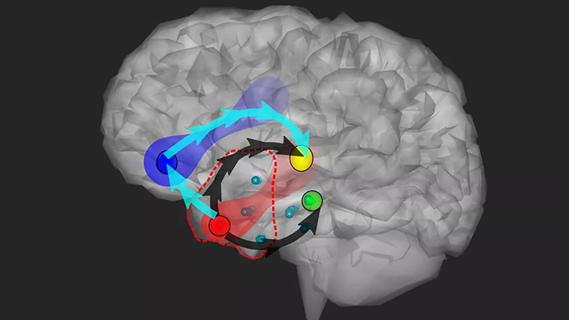
MRI showing an encephalocele (red arrow) and a widened Sylvian fissure (yellow arrows).
The clinical implications of identifying these lesions are substantial. In this study, 80% of patients achieved a favorable seizure outcome (International League Against Epilepsy [ILAE] classes 1-3) following resection, with 50% achieving complete seizure freedom (ILAE class 1).
Interestingly, the study challenged the traditional view that larger encephaloceles are more likely to be epileptogenic. The researchers found no direct correlation between lesion volume and seizure severity. This was most evident in a subset of six patients with bilateral encephaloceles. In most of these cases, the larger lesion was actually on the nonsurgical side, yet targeting the side with the higher tethering metrics (i.e., wider frontotemporal aperture and opercular angle difference) led to favorable outcomes. “This suggests that bilateral lesions are not a contraindication to unilateral surgery, provided the epileptogenic side is correctly identified through these novel markers,” Dr. Serletis observes.
Pathological review of the resected tissue revealed subpial gliosis or perivascular inflammation in 84% of cases and cortical dysplasia in nearly half of the patients. “This underscores that the encephalocele does not just cause focal irritation but may lead to more widespread neocortical disorganization,” Dr. Serletis notes.
Advertisement
The study authors note that their findings yield several key takeaways for the diagnostic workup of temporal lobe epilepsy:
“By integrating these metrics of frontotemporal aperture and opercular angle into standard radiological reviews, epilepsy teams can move closer to unmasking the cause of lesion-negative epilepsy and offering targeted, life-changing surgical interventions to a broader array of patients,” Dr. Serletis concludes.
Advertisement
Advertisement

Data-driven segmentation approach shows promise for seizure characterization with utility for clinical decision making

Insights from one of the first studies of invasive monitoring in the rare form of focal cortical dysplasia

Novel Cleveland Clinic project is fueled by a $1 million NIH grant

Patients with epilepsy should be screened for sleep issues

Sustained remission of seizures and neurocognitive dysfunction subsequently maintained with cannabidiol monotherapy

Model relies on analysis of peri-ictal scalp EEG data, promising wide applicability

Investigational gene approaches offer hope for a therapeutically challenging condition
Study combines intracranial electrophysiology and SPECT to elucidate the role of hypoperfusion