Locations:

Insights from one of the first studies of invasive monitoring in the rare form of focal cortical dysplasia
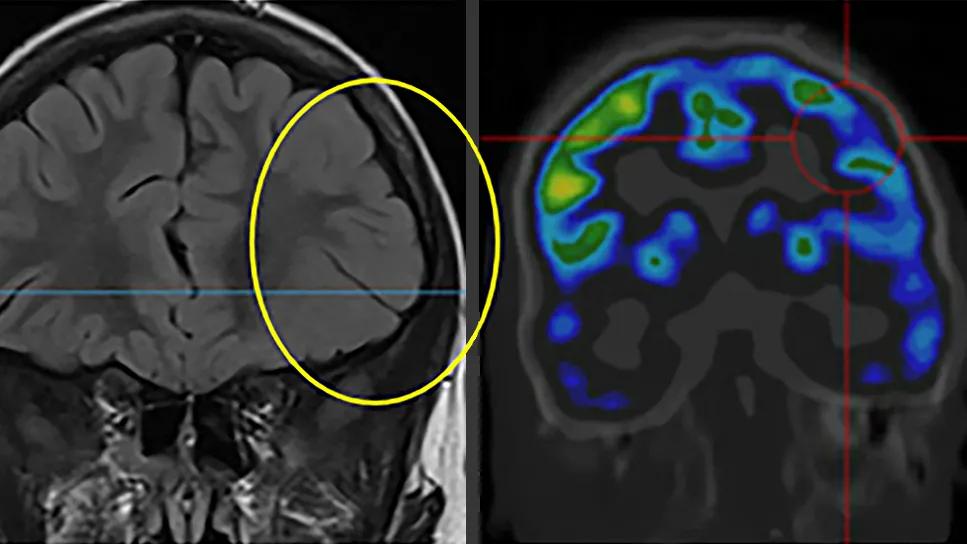
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/df9c1e34-f27f-4e5a-9db9-b3db6c71e623/brain-scans-study-of-moghe-epilepsy)
two brain scans side by side with a yellow circle on the left scan
Stereoelectroencephalography (SEEG) adds clear incremental value to neuroimaging and noninvasive EEG for delineating the epileptogenic zone with better spatial resolution in patients with medically refractory epilepsy due to mild malformation of cortical development with oligodendroglial hyperplasia (MOGHE), according to a new Cleveland Clinic study. SEEG helped identify larger epileptogenic zones than those suggested by imaging, which may result in more complete resection and higher seizure freedom rates following epilepsy surgery in these patients.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
The findings, published in Epilepsia (2026 Epub 2 Feb), are from a retrospective analysis comparing surgical outcomes among MOGHE patients who underwent standard preoperative assessment with scalp video-EEG and neuroimaging alone versus the standard assessment plus SEEG.
“This is the first detailed electroclinical characterization of surgically treated MOGHE patients,” says Cleveland Clinic epileptologist Jean Khoury, MD, the study’s first and corresponding author. “It shows that SEEG is beneficial for defining resection margins and suggests that optimal outcomes in this population may be linked to more complete resection of the ictal zone.”
First described in 2017, MOGHE is a rare subtype of focal cortical dysplasia that involves the juxtacortical white matter without significant histopathological cortical abnormalities. Pathology reveals heterotopic neurons in white matter, oligodendroglial cell hyperplasia with excessive proliferation, and patchy hypomyelination.
Patients with MOGHE typically develop drug-resistant focal epilepsy at a median age of 3 to 5 years, but the reasons why are unknown. Limited outcomes data from small series suggest that, in some cases, surgery may be effective. However, accurately delineating and localizing the epileptogenic zone with noninvasive techniques is challenging in the setting of MOGHE, and the role of invasive extraoperative monitoring is ill defined.
“At Cleveland Clinic, we’re seeing MOGHE in an increasing number of young patients undergoing surgery for epilepsy,” says Dr. Khoury. “Our objective was to understand the abnormality more fully and determine whether we can tailor resection for better outcomes.”
Advertisement
The study cohort comprised 23 patients surgically treated for epilepsy at Cleveland Clinic from 1997 to 2024 who had pathologically confirmed MOGHE. Demographic information and data on electroclinical features, surgeries (lesionectomies, partial lobectomies or subtotal lobectomies) and postoperative outcomes were extracted from patients’ electronic medical records.
Seizure data — available for all but one of the patients — was categorized based on frequency. Results of brain MRI and [18F] fluorodeoxy-glucose PET scans also were assessed.
All patients underwent presurgical scalp video-EEG, and 10 (43%) also underwent SEEG evaluation. Indications for SEEG were absence of a lesion on MRI, discordant or nonlocalizing ictal EEG patterns and delineation of the epileptogenic zone in MRI-positive cases.
From the SEEG patients, the authors reviewed electrode implantation maps and interictal and ictal EEG results, including videos of seizures.
Median ages at seizure onset and at surgery were 5 and 24 years, respectively, in the cohort overall. Seizure frequency was daily in 43% and weekly in 26%. Seizure semiology was focal in 83% of patients, with or without secondary bilateral tonic-clonic seizures.
In the SEEG subgroup, median age was 26.5 years and median epilepsy duration was 15.5 years.
MRI findings were abnormal in 83% of patients, but half the studies had initially been reported as normal. Gray-white matter blurring was the most common finding (74%), followed by cortical thickening (42%) and white matter changes (21%).
Advertisement
“The MRI features of MOGHE are subtle, and the most common is gray-white matter blurring,” Dr. Khoury notes. “This highlights the need for detailed review of dedicated high-resolution MRI studies in these patients by an expert neuroradiologist who specializes in epilepsy.”
Sixty-five percent of patients had generalized interictal EEG findings. Median duration of epilepsy was 8 years in those with generalized interictal epileptiform discharges, versus 21 years in patients without the discharges.
More than half of the surgeries (57%) were performed in the frontal lobe, 17% in the temporal lobe and 9% each in the temporo-parietal, temporo-occipital and parieto-occipital regions.
At median postoperative follow-up of 3.8 years, 64% of patients overall were seizure-free. Seizure freedom (Engel class I) was achieved in 80% of those who underwent SEEG versus 50% who did not undergo the procedure.
Looking at resection type, SEEG guidance and the lobe involved, the authors found a 90% seizure freedom rate in patients with SEEG-guided partial lobectomies. Postoperative seizure freedom also was seen in two patients who underwent SEEG-guided subtotal lobectomies.
A comparison of outcomes across resection types showed a trend toward better outcomes with larger resections, but the differences were not statistically significant.
“The role of SEEG guidance was particularly notable, as those patients who underwent SEEG-guided resections showed better outcomes as compared with non-SEEG cases,” says Dr. Khoury. “These findings were somewhat unexpected and indicate the significant contribution of SEEG-based definition of the epileptogenic zone. The difference in favor of SEEG is not usually seen in patients with a lesional MRI, underscoring the challenges of noninvasive localization in the setting of MOGHE.”
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/95539898-93b6-45c0-892e-d0437c0b4f38/brain-scans-study-of-moghe-epilepsy-inset)
Imaging and SEEG findings from a pediatric patient with MOGHE, which is seen on MRI in the top left image (circle). The combination of noninvasive testing and SEEG helped delineate the patient’s epileptogenic zone, leading to a complete surgical resection and seizure freedom without deficits.
According to the study authors, the findings highlight the clinical potential of SEEG for optimizing surgical planning and decision-making in patients with MOGHE, particularly when results of noninvasive imaging are discordant and/or imaging findings are subtle. “The epiltogenic zone in MOGHE often extends beyond MRI-visible lesions, necessitating tailored surgical strategies,” they write.
“Not every MOGHE patient needs SEEG, but our results underscore the limitations of relying solely on neuroimaging and noninvasive EEG modalities for presurgical planning,” says Dr. Khoury. “Further studies are needed to identify cases in which the technology would be most beneficial in this setting, because with this form of epilepsy, larger resection usually leads to better outcomes.”
Advertisement
Advertisement

Data-driven segmentation approach shows promise for seizure characterization with utility for clinical decision making

Early identification of temporal encephaloceles can improve surgical decision-making

Novel Cleveland Clinic project is fueled by a $1 million NIH grant

Patients with epilepsy should be screened for sleep issues

Sustained remission of seizures and neurocognitive dysfunction subsequently maintained with cannabidiol monotherapy

Model relies on analysis of peri-ictal scalp EEG data, promising wide applicability

Investigational gene approaches offer hope for a therapeutically challenging condition
Study combines intracranial electrophysiology and SPECT to elucidate the role of hypoperfusion