Locations:

Two cases — both tremendously different in their level of complexity — illustrate the core principles of nasal reconstruction

Patients may require nasal reconstruction for a variety of reasons, and the complexity can vary tremendously from case to case. The following two case studies are representations of both ends of the spectrum. One is a more straight-forward reconstruction, and the other is an extraordinarily challenging one. However, both cases represent similar principles in regard to reconstruction approach, technique and challenges. The Chair of Cleveland Clinic’s Head & Neck Institute, Patrick Byrne, MD, MBA, was the lead surgeon in both cases.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
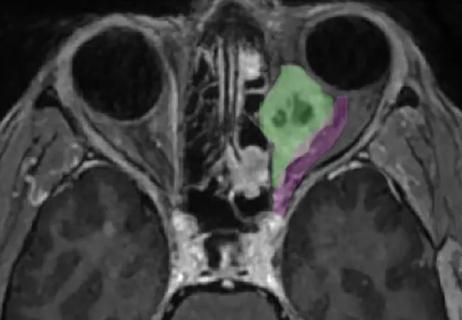
Patient A was a middle-aged woman with concerns about a growth on her nose. Several years prior, the patient had an instance of squamous cell carcinoma (SCC) on her eyelid, which required removal by a dermatologist. Dr. Bryne helped reconstruct the eyelid and eventually did a cosmetic eyelift and facelift as well. She visited her local dermatologist who felt that the growth on her nose was nothing of concern, but the patient convinced the dermatologist to perform a biopsy because of her skin cancer history. The growth came back positive for SCC. The patient decided to seek out a place to have Mohs surgery to remove the cancer and wanted a place where the reconstructive surgery would incorporate a team approach. This led her to Cleveland Clinic.
Allison Vidimos, MD, performed the Mohs surgery, which produced two defects on her nose, Dr. Byrne and his team had to devise a repair that would both close those holes and preserve the aesthetic structure of the nose.
“What made this case particularly challenging is that the skin requiring removal was on the nose,” says Dr. Byrne. “The nose is really the central feature of the face, and unfortunately, unlike almost anything else on the body, we can’t camouflage or cover it in any way. It is unforgiving, in that any tension on closure can distort the shape and position of the nose. It’s three-dimensional and complex, and even very small asymmetries are easily visible to observers. In some cases, the surgeon may have to remove much more than just the skin and remove the deeper structures as well. This becomes much more complex. However, I have learned to have great respect even for small skin defects only. If you are not really careful, these can leave patients deformed for life.”
Advertisement

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/3bf6530b-85f0-4ebc-8f7c-c0dbcf9fe3bf/22-HNI-3352902-NasalReconstruction-inset1_800x611_jpg)
Patient A before and after
It’s important to take skin cancer seriously, especially when a patient has a history of skin cancer. Cleveland Clinic supports a multidisciplinary approach where patients with skin cancers on their faces are treated by highly specialized experts. This includes dermatologists, Mohs surgeons and facial plastic surgeons.
Mohs surgery is a valuable technique for dermatologists, and it’s one of the most effective treatments for patients with cancer on their face. Not only is it able to remove the cancer, but it also leaves as much skin as possible, which makes the next steps easier for the reconstructive surgeon.
Mohs surgery for skin cancers on the nose remove skin in all cases. Sometimes the deeper structures require removal (an example of the reconstructive surgery strategy for more complex defects is presented below).
Skin defects (or, “holes”) on the nose are managed in one of three ways. Smaller defects can often be managed with what we call “local flaps”, or “adjacent tissue transfer.” This involves moving the surrounding nasal skin and stretching it to cover the defect. There are ingenious designs to do so without causing undue tension, avoiding distortions of the nasal shape, and making the resulting scars less obvious. The great advantage of local flap closures is that since the defect is closed with nasal skin, it is a perfect match.
However, there are times in which the defect is so large, that there just isn’t enough nasal skin to close it without causing a significant secondary deformity: a distorted or twisted nose. A common cutoff for this decision is a skin defect size between one and two cm. In those cases, skin must be brought to the nose from another site. This can be done via a skin graft (a free piece of skin transplanted onto the nose to cover the defect) or via an “interpolated flap”. Interpolated flaps involve a multi-stage procedure in which skin is brought down from the forehead, or over from the cheek, to cover the defect. It is left attached to its site of origin for several weeks. Then, once a new blood supply has been established in the nose, the connection to its original donor site is severed, and the nose (and donor site) is stitched close.
Advertisement
“The patient is doing terrific now — she says you can’t even tell she had anything done, and that’s really the goal with skin cancer patients,” says Dr. Byrne. “I want to get them to the point where other people no longer notice anything and the patient is no longer thinking about it either. I would say that in at least 85% of cases, regardless of the size of the defect, we can get patients to that point.”
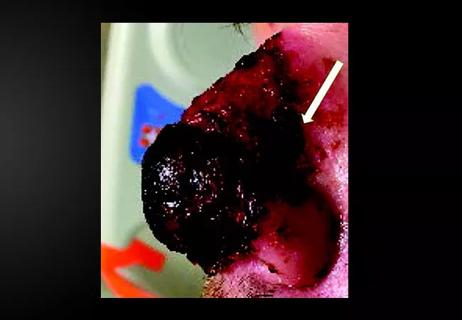
Patient B was a young man who suffered a traumatic amputation of, essentially, his entire nose. The accident occurred several years prior to presenting at Cleveland Clinic. After meeting with Dr. Byrne, reconstruction efforts began. The nose needed to be built almost entirely from scratch using the patient’s own tissue — cartilage from his ribcage, cartilage and skin from his ear, and tissue from his forehead for the external skin. Over several surgeries, Dr. Byrne and his team created an aesthetic and functional nose for the patient.
The nose was reconstructed in three layers. The internal layer needs to be thin and vascular. The middle layer, which is the structural layer, is composed of cartilage and bone. This layer, which is often referred to as the subsurface framework, essentially needs to be a three-dimensional sculpture that looks like a nose — but slightly miniaturized. The third layer is the external layer of skin —often this skin is taken from the forehead because it’s an excellent match in terms of tissue color and characteristics in most patients. “While there is no such thing as a simple nasal reconstruction, the larger the defect, typically the more complicated the case is, and total nasal reconstruction such as this case probably as difficult an endeavor as any in plastic surgery.” says Dr. Byrne.
Advertisement
In this case, the patient’s journey was even more difficult than usual. The patient suffered postoperative complications due primarily to infection. The infection resulted in resorption of much of the patient’s subsurface cartilaginous framework. “This can turn an initially good result into a complete disaster,” says Dr. Byrne. “I’ve learned over the years to take these early complications very seriously and act quickly whenever possible. Ultimately, we had to resort to the extraordinary measure of doing a second forehead flap to achieve an acceptable outcome.”
Eventually, the patient and the surgical team were able to get to the point where the nose is fully functional and aesthetic.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e37c4e37-893f-4937-bc25-fdabdaed66e6/22-HNI-3352902-NasalReconstruction-inset2_800x611_jpg)
Patient B before and after
The psychological impact of both the traumatic injury to the nose and the challenging reconstruction cannot be understated. Having a facial feature partially or completely removed is psychologically devastating. This type of injury radically changes a person’s appearance overnight. In this case, it was a traumatic injury, but more commonly, these result from cancer, as illustrated in the first case.
“We are usually able to re-create a relatively normal-looking nose and rehabilitate patients back to their normal lives. This helps them rebuild their confidence,” says Dr. Byrne. “However, this is invariably a long journey, requiring multiple procedures. Most people do not develop complications, but when they do, such as in this patient, one’s resolve is severely tested. I’ve learned over the years that success in reconstructive surgery is as much a function of skill and experience as it is of dogged determination. We’ve learned that with meticulous planning, attention to detail, patience and persistence, over time we can usually create something beautiful and functional out of the worst starting point.”
Advertisement
Advertisement

Despite advancements in the specialty, patient-centered care needs to remain a priority
By using free vascularized fascia lata flaps, surgeons can overcome some of the aesthetic and functional challenges historically associated with nasal reconstruction

Prompt, multidisciplinary care helps navigate the complexities of a rare condition
Novel collaborative approach helps patient avoid orbital exenteration

Family history may eclipse sun exposure in some cases

Consider secondary syphilis in the differential of annular lesions

Persistent rectal pain leads to diffuse pustules
Stress and immunosuppression can trigger reactivation of latent virus