Locations:

Pancreas and spleen removed to minimize risk of pancreatic cancer

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/468fca42-738d-480a-b0a2-c695e0b49c7e/22-DDI-3463613-Pancreatic-Cancer-Case-Study650x450-pancreas_jpg)
pancreas
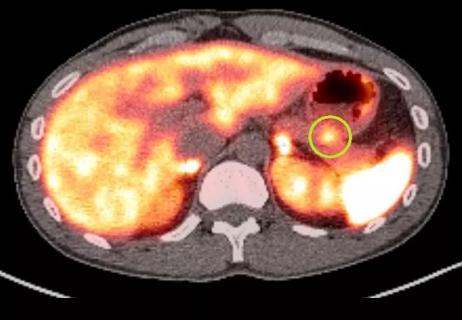
When a 58-year-old man notified his primary care provider that he was experiencing abdominal pain and was seeing what looked like oil in the toilet when he had a bowel movement, she ordered a CT scan. The patient was experiencing exocrine pancreatic insufficiency, resulting in oily stools due to fat malabsorption. The CT revealed a cyst on the pancreas and to further characterize it, his doctor referred him to gastroenterologist Amit Bhatt, MD, who followed up with an endoscopic ultrasound. This revealed main duct intraductal papillary mucinous neoplasm (IPMN), a benign pancreatic cyst. These cysts are a risk factor for developing into pancreatic cancer. While the diagnosis was frightening, when the disease is caught early, as in this case, it significantly improves the chances of a positive outcome.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
In most instances, IPMN is not treated operatively. Instead, it is monitored closely with frequent imaging. A set of guidelines is used to determine if IPMNs are more likely to be good actors or bad actors, and for those bad actors, a distal pancreatectomy or a whipple procedure can be performed to remove the risky lesions. In this case, the patient’s cyst was discussed amongst a multidisciplinary team, involving the pancreatic surgeon Robert Simon, MD, oncologist Bahar Laderian, MD, and gastroenterologist Amit Bhatt, MD, and deemed to be more likely to be a bad actor. Therefore, the consensus was to have it removed. The unusual part of his case is that it involved the entire pancreas and therefore, a total pancreatectomy with a splenectomy was required in order to remove it.
The surgery itself took approximately six hours and went well. The patient’s recovery was uneventful. He was discharged from the hospital after about a week. The entire specimen was analyzed by the pathologists, and there was a small (0.5cm) focus of adenocarcinoma found in the pancreas. “It was caught early and had not metastasized to the lymph nodes,” says Dr. Simon.
After the surgery, the patient’s case was brought back to the multidisciplinary team, and the recommendation was that in order to give the patient the best chance at survival, he should receive the triple-drug regimen FOLFIRINOX. As soon as the patient consented to the treatment, the Cleveland Clinic team, including pharmacists and infusion nurses, set to work behind the scenes to provide a swift time to treatment. This included preparing the patient to have a port placed to receive the chemotherapy and planning the infusion schedule.
Advertisement
A social worker was also assigned to help the patient with the emotional challenges of his long journey. “I think a social worker is really essential for complete cancer care,” says Dr. Laderian. “They are genuinely there to help everyone, the patient, their family and their care team.”
The patient struggled with fatigue, nausea and vomiting through the chemotherapy treatment, and his medical team worked closely with him to keep tabs on his symptoms and prescribe medications to alleviate his symptoms. Ultimately, he completed ten cycles of FOLFIRINOX. After finishing chemotherapy, he receives periodic scans and blood tests to check for tumor markers.
Since the patient is now living without a pancreas, he does need to control his blood sugar with insulin. After he recovered from surgery, he connected with an endocrinologist near his home in Tuscarawas to learn how to manage his diabetes. He was also prescribed specific enzymes that are important for digestion, as well as vaccines to protect against some bacterial infections, such as pneumonia, now that his spleen is gone.
More than a year and a half post-surgery, the patient is doing well and has no signs of recurrent cancer. He has returned to work part time, and enjoys numerous endeavors, such as playing the bass in a rock band.
“This case highlights the importance of patients listening to their bodies, noticing possible warning signs and connecting with their care team so symptoms can be investigated,” said Dr. Simon. He adds, “It is also imperative to go to a center that has specialists familiar with taking care of pancreatic diseases, such as cysts, as there are a lot of subtleties, and you want a care team who can help you make the right decision.”
Advertisement
Advertisement

Insulin use at time of hospital discharge can offer clues for the future

Patients spent less time in the hospital and no tumors were missed

A review of current evidence and recommendations

Findings indicate clinical decision making should not be driven by initial lesion size
Patient’s unexplained low blood glucose levels in the absence of diabetes spark quest for answers

Patients on ibrutinib were more than twice as likely to experience atrial fibrillation or heart failure than those on second-generation alternatives.

Expert recommendations introduce use of targeted agents

Combination therapy may soon represent new standard of care