Locations:

When a patient failed to improve, the value of a comprehensive vestibular test was apparent

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/4e573c45-dfc3-4c02-95f5-daaf37f15a7a/22-HNI-3464022-VestibularTestingRehab-CaseStudy-HonakerBehr-CQD-1_650x450_jpg)
vestibular testing
A 59-year-old female presented to Cleveland Clinic Head and Neck Institute for a vestibular test battery (VTB) evaluation. She had a history of left-sided sudden hearing loss with associated room-spinning vertigo lasting two days. She completed an audiologic evaluation, which revealed left ear hearing sensitivity within normal limits through 3000 Hz, sloping to severe sensorineural hearing loss (SNHL); right ear hearing sensitivity was within normal limits (see Figure 1). Word recognition abilities were considered “good” bilaterally. Tympanometry revealed normal tympanic membrane mobility bilaterally.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
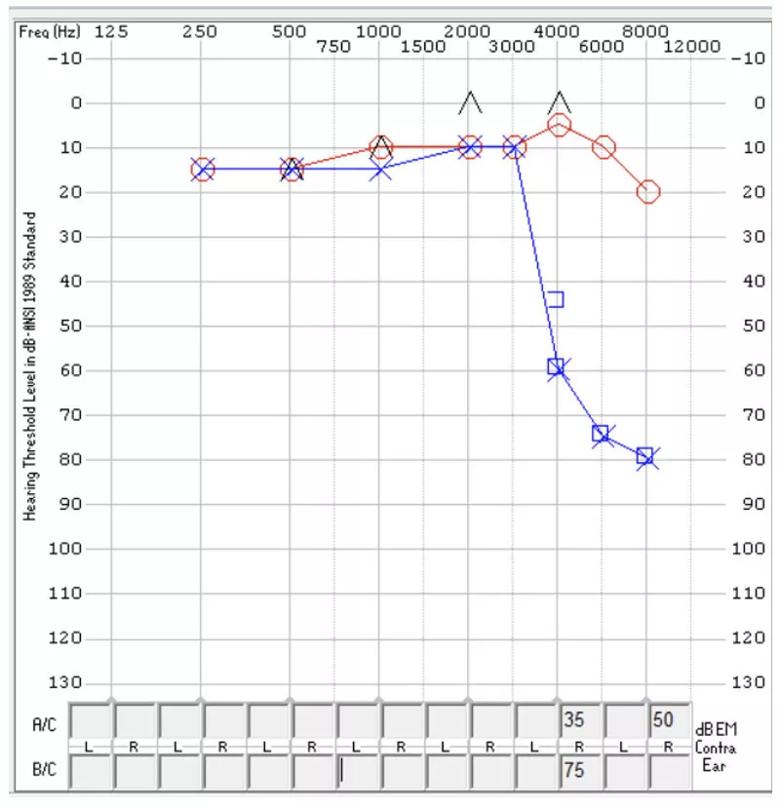
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/46d87a85-a2eb-4351-be37-72bfaf725f2b/22-HNI-3464022-VestibularTesting-RehabCaseStudy-inset_800x829-2_jpg)
Figure 1. The patient’s hearing sensitivity following of vertigo episode. The y-axis represents intensity level of sound measured in decibels (dB HL). Soft sounds are found at the top of the graph (-10 dB HL), with louder sounds at the bottom (130 dB HL). The x-axis represents the frequencies of sound measured in hertz (Hz). Low-frequency sound is near the left portion of the graph with the highest frequencies at the right. The red circles represent right ear hearing, while the blue “X’s” represent the left ear. Based on normative data, this patient has normal hearing in the right ear. The left ear hearing sensitivity is normal through 3000 Hz, sloping to severe sensorineural hearing loss.
Six months after the initial onset, she was referred for a vestibular evaluation as symptoms had not resolved despite medical management (multiple intratympanic steroid injections) and vestibular physical therapy. Vestibular testing was completed by vestibular audiologist, Evalena Behr, AuD. The exam was unremarkable apart from one test finding: The video head impulse test (vHIT) revealed left posterior semicircular canal (P-SCC) dysfunction with all other semicircular canals spared.
The vHIT isolates and measures the three semicircular canals (SCCs) in the vestibular labyrinth – the superior, horizontal and posterior canals – which are designed to encode angular acceleration across the roll, pitch and yaw planes. It was integrated into the clinical setting around 2016, which is perhaps why clinical trends are now emerging.
Advertisement
“When I investigated the medical literature regarding this clinical profile, a few articles suggested the presence of isolated P-SCC involvement could be a prognostic factor for hearing recovery in patients with sudden sensorineural hearing loss. The presence of isolated posterior canal involvement may suggest poor hearing recovery, which helps referring providers better understand hearing prognosis in this patient demographic,” explains Dr. Behr.
The patient’s sudden sensorineural hearing loss from 4000 – 8000 Hz may be due to an insult at the vestibulocochlear artery, which supplies the basal portion of the cochlea where high-frequency sound is encoded. The vestibulocochlear artery also exclusively supplies the posterior SCC. The superior and horizontal canal receive blood from the anterior vestibular artery, which would explain why the hearing loss was only present at the high frequencies and only the posterior SCC was impacted.
“We are seeing a unique clinical pattern of abnormal posterior canal function with normal function of all other SCCs. This pattern is often observed in patients with sudden hearing loss, suggesting a mechanistic link possibly supported by the proximity of inner ear neural and vascular structures,” states Dr. Behr.
However, more research is still necessary to fully understand these observations.
“We currently have an open prospective clinical study aimed to better understand the association between unilateral and bilateral posterior canal dysfunction and hearing loss and increased age,” says Julie Honaker, PhD, Section Head of Audiology at Cleveland Clinic.
Advertisement
This patient completed four sessions of vestibular rehabilitation (physical therapy) without resolution of symptoms before receiving a comprehensive vestibular evaluation.
In this case, the VTB provided crucial information to help guide physical therapy (PT) with appropriate treatment. For vestibular compensation (adaptation) to take place at the level of the cerebellum and brainstem after a vestibular lesion, head and body movement is necessary for the plane corresponding to the impaired SCC. The posterior canal decodes motion in the roll and pitch plane, and the patient was completing exercises in the horizontal plane, which is likely why the patient was not progressing through PT as expected.
After completing the VTB, the patient returned to physical therapy with vestibular physical therapist, Tod Kokensparger, PT. The patient’s treatment regimen was altered to include vertical head movements to facilitate vestibular compensation of the posterior canal. Using the information obtained from the VTB, the patient continued to progress toward physical therapy goals.
This case demonstrates the importance of patients receiving a VTB – especially if symptoms persist despite multiple sessions of PT – and the value of a comprehensive vestibular evaluation.
Advertisement
Advertisement

How a new clinic is helping to streamline evaluations for patients
Subtle information gleaned from clinical examinations prompted concern

A comprehensive evaluation and multidisciplinary care are key to caring for patients with vestibular disorders

Innovative approach to the procedure can yield significant relief in complex cases

Study shows no negative impact for individuals with better contralateral ear performance

Effective screening, advanced treatments can help preserve quality of life

Auditory hallucinations lead to unusual diagnosis

Expanded patient criteria and surgical advances mean more patients can benefit