Locations:

Pulmonary endarterectomy plays central role in era of multimodal therapy
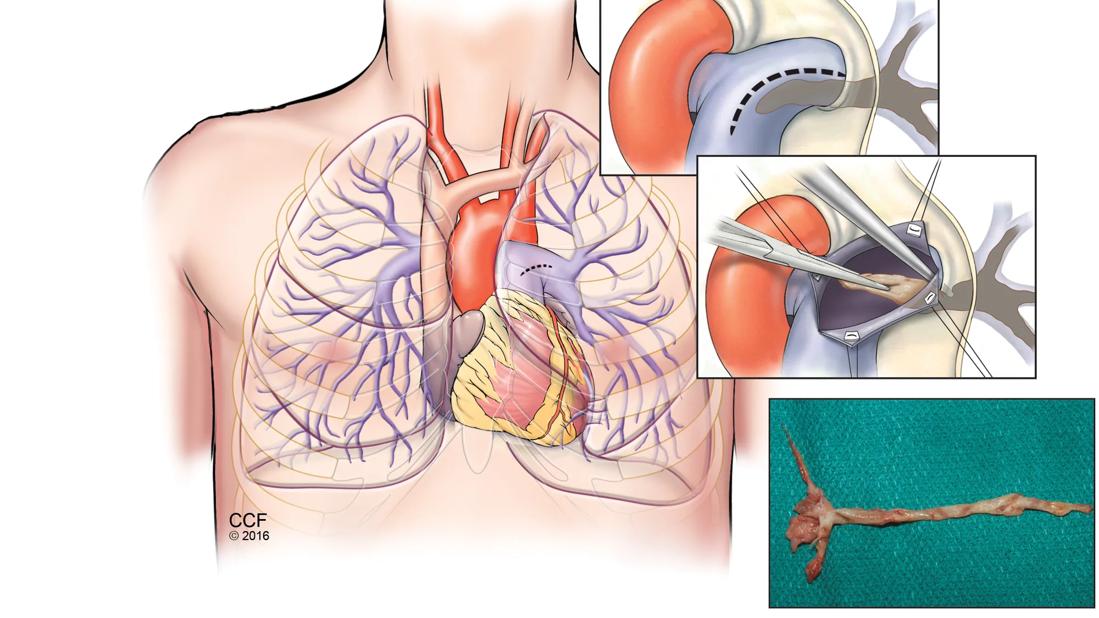
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e9c5b9b1-32c4-4195-91f5-25e9afd09ee1/Pulmonary-endarterectomy-surgery-CTEPH)
Chronic Thromboembolic Pulmonary Hypertension: From Early Recognition to Curative Surgery
Chronic thromboembolic pulmonary hypertension (CTEPH) is a distinct and potentially curable form of pulmonary hypertension caused by persistent obstruction of the pulmonary vasculature by organized thrombi, often following acute pulmonary embolism. Despite its treatability, diagnosis is frequently delayed, contributing to progressive right ventricular dysfunction and avoidable morbidity.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Advances in diagnostic criteria, imaging, surgical technique, and multimodal therapy have reshaped the management landscape in recent years, reports cardiothoracic surgeon Nicolas A. Brozzi, MD, Surgical Director of Mechanical Circulatory Support at Cleveland Clinic Weston Hospital and member of a multidisciplinary team responsible for evaluating and treating patients with CTEPH.
CTEPH results from chronic obstruction and remodeling of the pulmonary arteries due to organized clots and fibrotic tissue, leading to elevated pulmonary artery pressures and progressive right ventricular strain. Untreated, patients with CTEPH develop secondary injury to the non-obstructed pulmonary vasculature, resulting in a small-vessel vasculopathy similar to that seen in other forms of pulmonary arterial hypertension.
The 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) guidelines for the diagnosis and treatment of pulmonary hypertension introduced several updates directly relevant to CTEPH:
Advertisement
“These changes support earlier recognition and more consistent referral pathways,” states Roger Alvarez, DO, the Medical Director of the Pulmonary Hypertension and CTEPH programs at Weston Hospital. “Despite some improvement in diagnostic consistency since the updated guidelines were issued, we are still seeing a number of patients with a history of pulmonary embolism and persistent symptoms go undiagnosed for many years.”
Ventilation/perfusion (V/Q) scintigraphy remains the cornerstone screening modality for suspected CTEPH. However, contemporary practice increasingly integrates dual-energy CT pulmonary angiography with perfusion imaging, SPECT-CT, and, in select cases, MRI to better characterize lesion morphology, distribution, and surgical accessibility.
“With the complex CT scans that we have available today, we can better understand the extent and location of the disease, which helps with better preoperative planning for eligible patients,” explains Dr. Brozzi. “Better planning means we can be more accurate at the time of performing the surgery.”
Multimodal imaging not only refines operability assessment but may also streamline evaluation protocols, reduce unnecessary testing, and accelerate referral to expert CTEPH centers. “This may help address a longstanding contributor to underdiagnosis,” notes Dr. Alvarez.
Pulmonary endarterectomy (PEA), also known as pulmonary thromboendarterectomy, remains the first-line and potentially curative treatment for patients with operable CTEPH. It is recommended for individuals with surgically accessible disease – typically involving the main, lobar or segmental pulmonary arteries – after a comprehensive multidisciplinary evaluation.
Advertisement
PEA is performed at a limited number of expert centers in Florida, including Weston Hospital. “This is a technically complex procedure that typically lasts 5 to 8 hours, requiring a median sternotomy, cardiopulmonary bypass, and deep hypothermic circulatory arrest to create a bloodless operative field that allows complete removal of obstructive material from the pulmonary arteries,” explains Dr. Brozzi.
Recent advances have expanded the surgical reach to more distal disease, allowing successful treatment in patients previously deemed inoperable. With refined intraoperative classification systems and experienced teams, operative mortality at high-volume centers is approximately 2%. Patients experience significant symptom relief with improvement in quality of life, and long-term survival following PEA is excellent – approximately 90% at three years and 75% at 10 years.
In a recent case, a 79-year-old former firefighter presented with progressive fatigue and dyspnea. Despite significant right ventricular dilation and severe pulmonary hypertension, he remained in otherwise good clinical condition. “The patient’s right heart had significant dilatation and was struggling to keep up,” Dr. Brozzi recalls.
Bilateral pulmonary endarterectomy was performed, with complete removal of organized scar tissue from both pulmonary arterial trees. The patient was discharged five days later. At one-month follow-up, he reported full return to baseline functional status without limitation in activities of daily living – an excellent hemodynamic and clinical outcome.
Advertisement
Not all patients are candidates for PEA. For those with inoperable distal disease, persistent pulmonary hypertension after surgery, or prohibitive surgical risk, treatment options include balloon pulmonary angioplasty (BPA) and targeted medical therapy.
BPA is a staged, catheter-based intervention in which a balloon is inflated within affected pulmonary artery branches to widen the lumen by compressing obstructive material against the vessel wall. While it does not remove organized thrombus, it improves perfusion and hemodynamics. BPA is especially helpful in patients whose blockages are in the medium and small arteries, including those too deep in the lung to reach through surgery.
“This staged approach has dramatically reduced complication rates in recent years, although multiple sessions are typically required,” notes Dr. Brozzi.
Riociguat remains the only approved targeted pharmacologic therapy for inoperable CTEPH and has demonstrated benefit both before and after BPA. According to Dr. Alvarez, it has been shown to reduce worsening exercise intolerance and improve functional capacity in that patient population.
“While riociguat is a great tool, it can only improve blood flow in constricted small arteries, not the larger arteries suffering from blockages,” Dr. Alvarez notes. “So before starting a patient on riociguat, it is essential that they be evaluated for potential candidacy for surgery or angioplasty at a CTEPH center.”
Long-term anticoagulation is mandatory following any intervention for CTEPH. Ongoing surveillance is also essential, as recurrent or residual disease may necessitate additional medical, interventional or surgical management.
Advertisement
Pulmonary hypertension affects approximately 1% of the global population, and CTEPH is increasingly recognized as the only curable subtype, with up to 3,000 new cases diagnosed annually in the United States, according to the American Lung Association.
Earlier detection, expanded surgical indications, improved perioperative care, safer and more effective BPA, and hybrid treatment strategies have collectively improved survival and quality of life for both operable and inoperable patients.
For physicians, heightened awareness of persistent dyspnea after pulmonary embolism and early referral to an expert CTEPH center are critical steps. As demonstrated at Cleveland Clinic Weston Hospital, comprehensive multidisciplinary care – anchored by experienced medical and surgical expertise – offers patients the best opportunity for hemodynamic normalization, symptom relief, and long-term survival.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/e9c5b9b1-32c4-4195-91f5-25e9afd09ee1/Pulmonary-endarterectomy-surgery-CTEPH)
Figure 1: Pulmonary endarterectomy surgery relieves congestion of pulmonary arteries associated with CTEPH.

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/f9110ad3-18b7-48e7-b603-8c5b82d0f69f/thromboembolic-material-removed-from-pulmonary-arteries)
Figure 2: Surgical specimen showing thromboembolic material removed from pulmonary arteries (right upper -RUL-, middle-RML-, right lower -RLL- lobes, and left upper-LUL-, left lower-LLL- lobes).
Advertisement

Study highlights strong predictive value of circulating tumor DNA testing

Researchers with Cleveland Clinic in Florida highlight need for a national registry for gastrointestinal stromal tumors

Multidisciplinary LARS Center addresses life-altering consequence of rectal cancer surgery

Early recognition and intervention recommended in cubital tunnel syndrome

Manpreet (Meena) Bedi, MD, named Division Chair of Radiation Oncology

AR-assisted navigation is closing the gap between surgical planning and implant placement

Evidence shows early evaluation improves survival and quality of life – yet many eligible patients are referred too late

2026 ADA Standards of Care promote holistic, multisystem management