Locations:

Switching medications may decrease treatment burden and macular fluid

Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/b3a6e150-8fb7-4240-bf4f-aa619c7eecd3/EYE_3861946_05-05-23_186_LDJ-jpg)
Eye doctor looking into a man's eye
Intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections, including aflibercept, bevacizumab and ranibizumab, have significantly improved outcomes for patients with neovascular age-related macular degeneration (nAMD). However, some disease is resistant to anti-VEGF therapy, causing patients to have residual macular fluid or need frequent treatment.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
Approved by the U.S. Food and Drug Administration in 2022, faricimab is the latest agent to be added to the anti-VEGF class. The clinical trials for faricimab in age-related macular degeneration (AMD) were solely in treatment-naive patients, making it difficult to generalize and apply the data to real-world patients, says Sumit Sharma, MD, a retina and uveitis specialist at Cleveland Clinic Cole Eye Institute.
“We wanted to see how our treatment-resistant patients did when they were switched to faricimab after being treated with other agents,” he says.
The resulting study was published in Ophthalmology Retina.
The retrospective study assessed Cole Eye Institute patients with nAMD who had been treated with anti-VEGF injections and switched to intravitreal faricimab. A total of 126 eyes of 106 patients were included, with 87% switching from aflibercept.
“Aflibercept has been our top agent for patients with nAMD who are resistant to treatment with bevacizumab,” says Dr. Sharma.
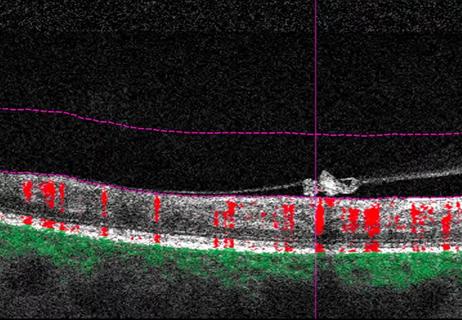
Central subfield thickness (CST), maximum pigment epithelial detachment (PED) height, and the presence of subretinal fluid (SRF) or intraretinal fluid (IRF) were evaluated on the first day of faricimab injection as well as after each treatment.
“The most important finding was that patients who were treatment-resistant on aflibercept — having persistent fluid or requiring treatment every four to six weeks — did a little better with faricimab,” says Dr. Sharma.
For most patients, faricimab increased the time between injections by one to two weeks. It also resulted in less macular fluid, as evidenced by a reduction in maximum PED height and mean CST, as well as an increase in patients without SRF or IRF after three injections. Visual acuity remained stable during treatment.
Advertisement
Although adding a week or two between injections may not seem like much, for patients needing injections every four weeks, the number of injections per year would decrease from 13 to eight or nine.
“That’s a significant reduction in treatment burden from the patient perspective,” says Dr. Sharma.
If the study had analyzed treatment-naive patients, a sizable portion may have been able to go 12 or 16 weeks between treatments, he notes.
“Anytime you switch medications, there’s a risk, and there were a few patients in our group who had inflammation after switching to faricimab,” adds Dr. Sharma. “Luckily, they were mild cases, and all of those patients did fine switching back.”
However, most of the 8.7% of patients who changed back to aflibercept did so because of worsening SRF or IRF.
For clinicians who switch their patients to faricimab, expect about 1 in 10 to go back to their original anti-VEGF agent, he says.
Dr. Sharma considers faricimab another tool in the armamentarium for treating nAMD.
“I think it’s worthwhile to consider faricimab in our patients if they’re treatment-resistant on aflibercept,” he says.
When counseling patients who are thinking of switching to faricimab, physicians should tell them to expect to see either less fluid or a slightly longer interval between treatments, advises Dr. Sharma. “But they shouldn’t expect to get out to 16 weeks if they’re currently on an every-four-week interval.”
Advertisement
Advertisement

New insights on effectiveness in patients previously treated with other anti-VEGF drugs

Evidence mounts that these diabetes and obesity drugs may protect eyes, not endanger them

CFH gene triggers the eye disease in white patients but not Black patients

A primer on sustained release options

Study explores association between sleep aid and eye disease
Early data show risk is 73% higher in patients with lupus, 40% higher in patients with rheumatoid arthritis
Why retina specialists should get comfortable with this imaging tool

Study identifies factors that may predict vision outcomes in diabetic macular edema