Locations:

Conservative treatments were ineffective for 29-year-old with chronic heel pain
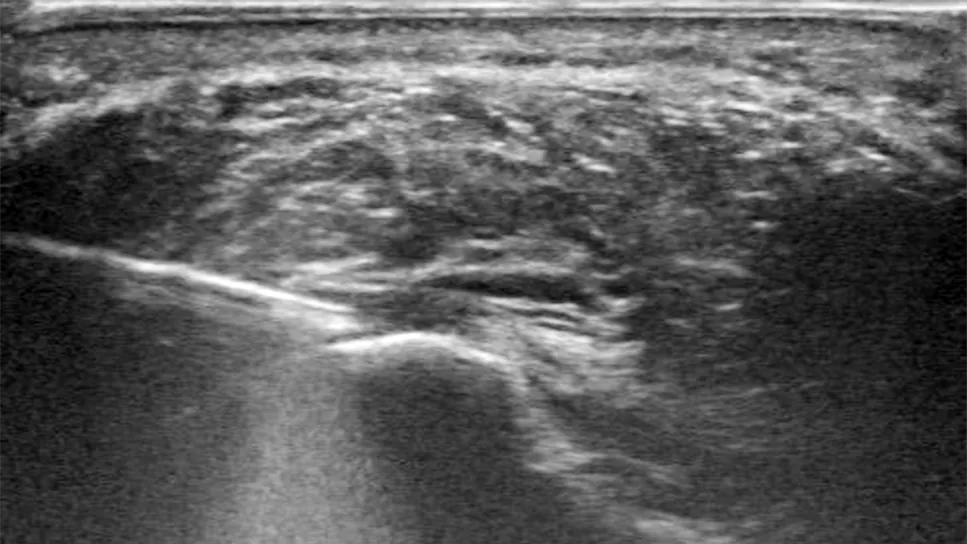
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/6b006560-b1df-4161-9d65-e5e2610846b2/TenJet-scan)
Hydroresection of plantar fascia
Shown above: Under ultrasound guidance, a slender hydroresection tool applies a pressurized, high-velocity stream of saline to debride diseased plantar fascia tissue.
Advertisement
Cleveland Clinic is a non-profit academic medical center. Advertising on our site helps support our mission. We do not endorse non-Cleveland Clinic products or services. Policy
A 29-year-old woman presented with bilateral heel pain that had been affecting her quality of life for nearly one year. She reported no inciting injury and had been diagnosed with plantar fasciitis.
First-line treatment — including oral anti-inflammatory medication, physical therapy, cortisone injections and night splints — did not control the pain. As a result, the patient had quit her job because she could no longer stand for hours a day. She also could no longer perform weight-bearing exercise, a concern because she had obesity and desired to increase physical activity.
“Plantar fascia pain can take up to one year to resolve and can be debilitating,” says Jason Genin, DO, an interventional sports medicine physician in Cleveland Clinic’s Department of Orthopaedic Surgery. “The chronic pain can exacerbate other conditions, as seen in this patient with obesity.”
Patients with refractory plantar fasciitis often are referred for surgical release of the plantar fascia. However, surgical outcomes can vary, and recovery can take months.
“Surgery comes with long-term considerations because it changes the structure of the feet, sometimes decreasing arch height and causing an altered gait,” adds Cleveland Clinic interventional sports medicine physician Vikas Patel, DO. “For these reasons, surgical release was not preferred for a young patient like this.”
Instead, the patient was referred for an interventional therapy, hydroresection. Using ultrasound guidance and a slender tool applying a pressurized, high-velocity stream of saline, the plantar fascia’s diseased tissue could be debrided in the office.
Advertisement
After positioning the patient, Dr. Patel used ultrasound to locate inflammation in the plantar fascia. (Tissue degeneration can cause areas of the plantar fascia to become hypoechoic, swollen with poorly formed collagen and water.)
Next, lidocaine and epinephrine were injected into the plantar fascia for anesthesia and to help control bleeding. Dr. Patel then made a tiny incision into which he inserted the hydroresection needle. The needle shot saline into the diseased, fibrotic tissue, resecting it while simultaneously using suction to remove it, leaving healthy tissue intact.
“It usually takes a couple of minutes to treat all the diseased spots we identify on ultrasound,” Dr. Patel says. “Patients may feel some pressure or nothing at all. Then we bandage the wound. No stitches are required.”
Some patients also require immobilization after the procedure. The patient in this case wore an immobilizing boot for two weeks.
All patients presenting at Cleveland Clinic with challenging tendinopathies, including plantar fasciitis, can benefit from the Tendon Evaluation and Arthritis Management (TEAM) program. Before an interventional procedure like hydroresection, every patient meets with a physical therapist along with their medical team in a combined appointment rather than scheduling a separate consultation with physical therapy after the procedure.
“We adapted this novel concept from Major League Baseball and have found that the coordination of care increases patient satisfaction and decreases burden,” says Dr. Genin, a team physician for the Cleveland Guardians. “The patient learns upfront what to expect each week after the procedure, what activity they will be allowed to do, how to wear their immobilization device and other details. All team members use the same language and follow the same plan, which helps alleviate confusion for patients.”
Advertisement
Three weeks after receiving hydroresection care as part of the TEAM program, the patient in this case was able to resume regular activities with no pain. She reported that she could stand or walk for hours and no longer felt intense pain when taking the first few steps after getting out of bed. She returned to work and was able to begin an exercise regimen to help reduce her body weight. Now 18 months later, she has lost 83 pounds.
“Every patient is different,” Dr. Patel says. “Some feel better immediately after treatment while others take a few weeks.”
Patients do not require follow-up care unless their pain returns.
Hydroresection can be an alternative to release surgery for patients with plantar fasciitis, rotator cuff issues and tendinopathy of all kinds (as seen in this figure).
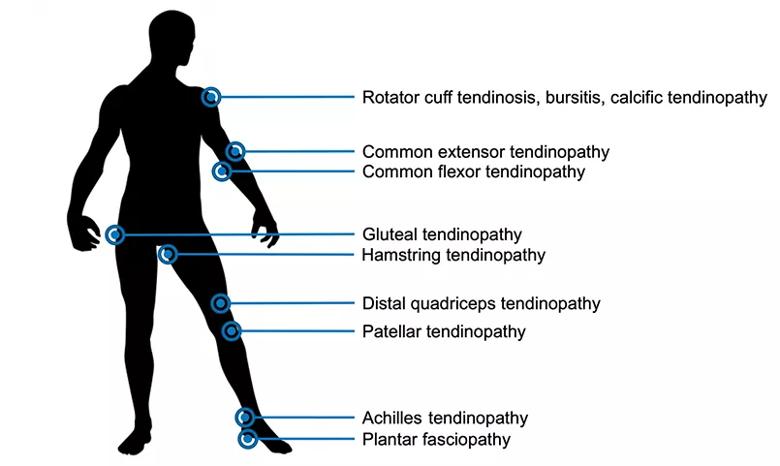
Image content: This image is available to view online.
View image online (https://assets.clevelandclinic.org/transform/899f2bcf-fa4e-4912-b7d6-425f0d19954b/21-ORI-2413859-tendinopathy-figure-Inset1_jpg)
Conditions treated by interventional therapies like hydroresection.
“Interventional therapies like hydroresection are a complement to orthopaedic surgery,” Dr. Genin says. “We don’t always need to open the body and remove the tendon. Sometimes we can work in a very small area, under ultrasound, to destroy just the diseased tissue while preserving the healthy tissue.”
Cleveland Clinic performs more than 500 interventional sports medicine procedures each year, including hydroresection and injections to treat chronic tendon pain.
“The patient in this case appeared to have only mild plantar fasciitis according to her diagnostic MRIs and ultrasound imaging,” Dr. Genin adds. “But even with mild findings, a condition still can have a major impact on quality of life. It led to job loss for this patient. This case exhibits how we can treat tendinopathies aggressively, offering patients long-term solutions without surgery.”
Advertisement
Advertisement

Confounding symptoms and a complex medical history prove diagnostically challenging

Surgeon corrects skew foot to address repeat injuries

Innovative procedure offers less-invasive alternative to Latarjet procedure

Even patients with reported penicillin allergies can receive it without increased complications

Study challenges assumptions about risk evaluation in total hip revision

Protein expression in synovial fluid indicates patients’ immune factors may be involved

Cleveland Clinic’s Global Peak Performance Center and PGA TOUR partnership pair advanced assessment with longitudinal follow-up to enhance clinical decision-making

Study highlights the need for objective functional measures as value-based care expands